
6 results
Carbapenem-resistant Acinetobacter baumannii and Carbapenem-resistant Enterobacterales in US Dialysis Populations, 2016-2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 4 / Issue S1 / July 2024
- Published online by Cambridge University Press:
- 16 September 2024, pp. s87-s88
-
- Article
-
- You have access
- Open access
- Export citation
-
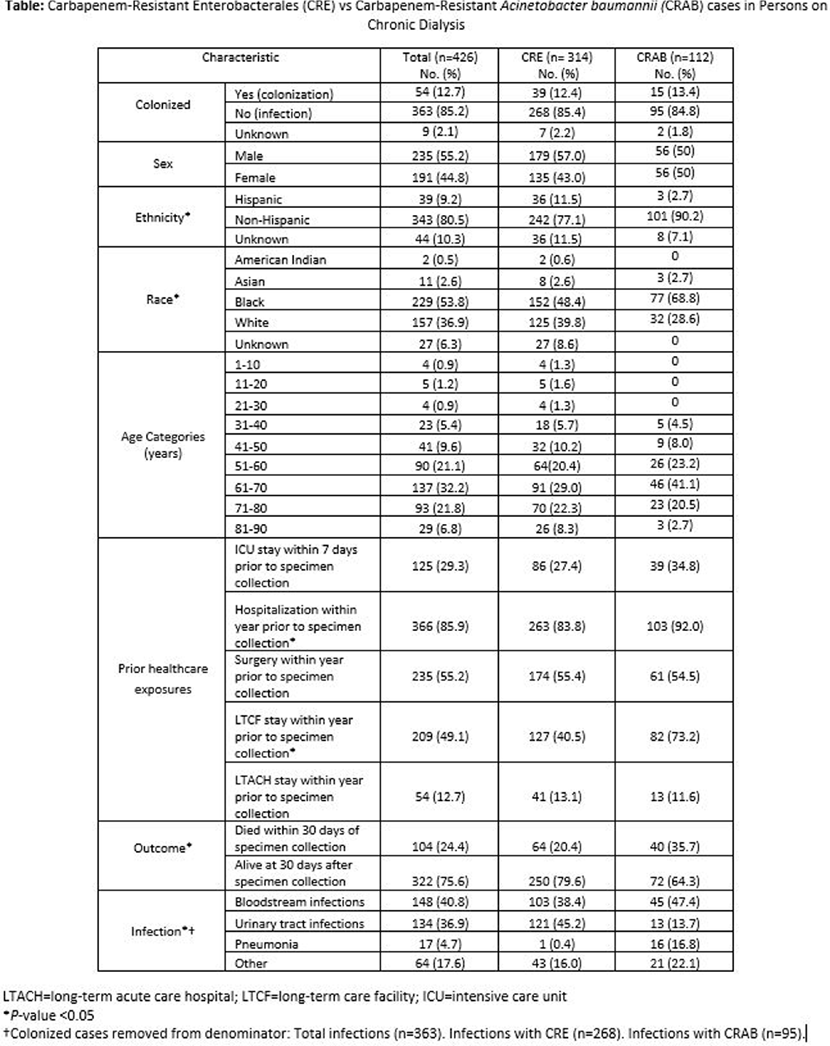
Background: Infections lead to high mortality among patients on chronic dialysis; knowledge of multi-drug resistant infections is limited. The Centers for Disease Control and Prevention’s Emerging Infections Program (EIP) conducts laboratory- and population-based surveillance for carbapenem-resistant Enterobacterales (CRE) in 10 U.S. sites and carbapenem-resistant Acinetobacter baumannii (CRAB) in 9 U.S. sites. We investigated clinical characteristics, healthcare exposures, and outcomes of CRE and CRAB cases in persons on chronic dialysis from 2016-2021. Methods: Among EIP catchment-area residents on chronic dialysis, we defined a CRE case as the first isolation of Escherichia coli, Enterobacter cloacae complex, Klebsiella aerogenes (formerly Enterobacter aerogenes), Klebsiella oxytoca, Klebsiella pneumoniae, or Klebsiella variicola resistant to any carbapenem, from a normally sterile site or urine in a 30-day period. A CRAB case was defined as the first isolation of Acinetobacter baumannii complex resistant to any carbapenem (excluding ertapenem), from a normally sterile site or urine (or lower respiratory tract or wound since 2021) in a 30-day period. Medical records were reviewed. A case was considered colonized if the case culture had no associated infection type or colonization was documented in the medical record. Descriptive analyses, including analyses stratified by pathogen, were conducted. Results: Among 426 cases, 314 were CRE, and 112 were CRAB; most cases were male (235, 55.2%), Black (229, 53.8%), and 51-80 years old (320, 75.1%) (Table). An infection was associated with 363 (85.2%) case cultures; bloodstream infections (148; 40.8%), urinary tract infections (134; 36.9%), and pneumonia (17; 4.7%) were the most frequent. Overall, most cases had documented healthcare exposures (excluding outpatient dialysis) in the year before incident specimen collection, including: 366 (85.9%) hospitalizations, 235 (55.2%) surgeries, 209 (49.1%) long-term care facility stays, 54 (12.7%) long-term acute care facility stays. Additionally, 125 (29.3%) had an intensive care unit admission within the 7 days before incident specimen collection. Compared to CRE cases, a higher proportion of CRAB cases (a) had a long-term care facility stay (82/112 [73.2%] versus 127/314 [40.5%], P<.0001) or hospitalization (103/112 [92%] versus 263/314 [83.8%], P = .03) within the preceding year and (b) died within 30 days of incident specimen collection (40/112 [35.7%] versus 64/314 [20.4%], P = .001). Discussion: Among CRE and CRAB cases in persons on chronic dialysis, healthcare exposures were common, and mortality was high. Additional efforts to better describe the burden of these organisms and associated risk factors in the dialysis population are needed for tailoring infection prevention strategies to this vulnerable.

Epidemiology of carbapenem-resistant and extended-spectrum beta-lactamase-producing Enterobacterales in US children, 2016–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s16
-
- Article
-
- You have access
- Open access
- Export citation
Epidemiology of extended-spectrum β-lactamase–producing Enterobacterales in five US sites participating in the Emerging Infections Program, 2017
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 11 / November 2022
- Published online by Cambridge University Press:
- 14 February 2022, pp. 1586-1594
- Print publication:
- November 2022
-
- Article
- Export citation
Characterization of Ceftazidime-Avibactam-Resistant Carbapenem-Resistant Enterobacteriaceae, United States, 2015–2017
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s465-s466
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Epidemiologic Characteristics of ESBL-Producing ST131 E. coli Identified Through the Emerging Infections Program, 2017
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s214-s215
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Area-Based Socioeconomic Status Measures and Incidence of Community-Associated ESBL-Producing Enterobacteriaceae, 2017
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s128-s129
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
