
103 results
546 Using Contingency Management to Understand the Cardiovascular, Immune and Psychosocial Benefits of Reduced Cocaine Use: A Protocol for a Randomized Controlled Trial
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 163
-
- Article
-
- You have access
- Open access
- Export citation
COVID-19 passenger screening to reduce travel risk and translocation of disease
-
- Journal:
- Epidemiology & Infection / Volume 152 / 2024
- Published online by Cambridge University Press:
- 08 February 2024, e36
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The origins of saddles and riding technology in East Asia: discoveries from the Mongolian Altai
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Testing the Effect of Information on Discerning the Veracity of News in Real Time
-
- Journal:
- Journal of Experimental Political Science , First View
- Published online by Cambridge University Press:
- 08 November 2023, pp. 1-15
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Management of routine postoperative pain for children undergoing cardiac surgery: a Paediatric Acute Care Cardiology Collaborative Clinical Practice Guideline
-
- Journal:
- Cardiology in the Young / Volume 32 / Issue 12 / December 2022
- Published online by Cambridge University Press:
- 16 November 2022, pp. 1881-1893
-
- Article
- Export citation
Laboratory-Based 3D X-ray Imaging of Neutron-Irradiated Ceramic Particle Nuclear Fuel
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 2038-2039
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Distributions on partitions arising from Hilbert schemes and hook lengths
- Part of
-
- Journal:
- Forum of Mathematics, Sigma / Volume 10 / 2022
- Published online by Cambridge University Press:
- 29 June 2022, e49
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
Recent works at the interface of algebraic combinatorics, algebraic geometry, number theory and topology have provided new integer-valued invariants on integer partitions. It is natural to consider the distribution of partitions when sorted by these invariants in congruence classes. We consider the prominent situations that arise from extensions of the Nekrasov–Okounkov hook product formula and from Betti numbers of various Hilbert schemes of n points on
 ${\mathbb {C}}^2$
. For the Hilbert schemes, we prove that homology is equidistributed as
${\mathbb {C}}^2$
. For the Hilbert schemes, we prove that homology is equidistributed as
 $n\to \infty $
. For t-hooks, we prove distributions that are often not equidistributed. The cases where
$n\to \infty $
. For t-hooks, we prove distributions that are often not equidistributed. The cases where
 $t\in \{2, 3\}$
stand out, as there are congruence classes where such counts are zero. To obtain these distributions, we obtain analytic results of independent interest. We determine the asymptotics, near roots of unity, of the ubiquitous infinite products
$t\in \{2, 3\}$
stand out, as there are congruence classes where such counts are zero. To obtain these distributions, we obtain analytic results of independent interest. We determine the asymptotics, near roots of unity, of the ubiquitous infinite products
 $$ \begin{align*}F_1(\xi; q):=\prod_{n=1}^{\infty}\left(1-\xi q^n\right), \ \ \ F_2(\xi; q):=\prod_{n=1}^{\infty}\left(1-(\xi q)^n\right) \ \ \ {\mathrm{and}}\ \ \ F_3(\xi; q):=\prod_{n=1}^{\infty}\left(1-\xi^{-1}(\xi q)^n\right). \end{align*} $$
$$ \begin{align*}F_1(\xi; q):=\prod_{n=1}^{\infty}\left(1-\xi q^n\right), \ \ \ F_2(\xi; q):=\prod_{n=1}^{\infty}\left(1-(\xi q)^n\right) \ \ \ {\mathrm{and}}\ \ \ F_3(\xi; q):=\prod_{n=1}^{\infty}\left(1-\xi^{-1}(\xi q)^n\right). \end{align*} $$




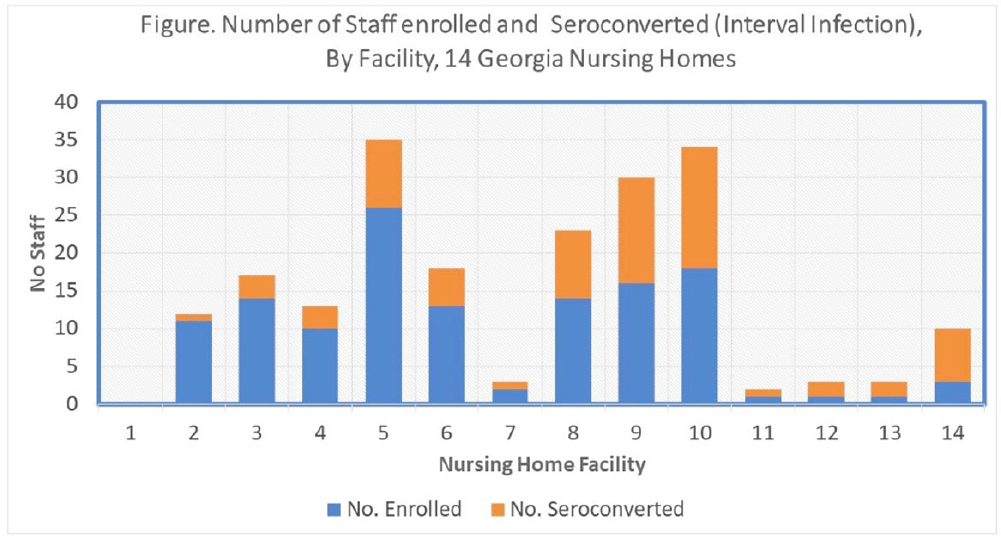
Which nursing home workers were at highest risk for SARS-CoV-2 infection during the November 2020–February 2021 winter surge of COVID-1?
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s7
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Nursing home (NH) residents and staff were at high risk for COVID-19 early in the pandemic; several studies estimated seroprevalence of infection in NH staff to be 3-fold higher among CNAs and nurses compared to other staff. Risk mitigation added in Fall 2020 included systematic testing of residents and staff (and furlough if positive) to reduce transmission risk. We estimated risks for SARS-CoV-2 infection among NH staff during the first winter surge before widespread vaccination. Methods: Between February and May 2021, voluntary serologic testing was performed on NH staff who were seronegative for SARS-CoV-2 in late Fall 2020 (during a previous serology study at 14 Georgia NHs). An exposure assessment at the second time point covered prior 3 months of job activities, community exposures, and self-reported COVID-19 vaccination, including very recent vaccination (≤4 weeks). Risk factors for seroconversion were estimated by job type using multivariable logistic regression, accounting for interval community-incidence and interval change in resident infections per bed. Results: Among 203 eligible staff, 72 (35.5%) had evidence of interval seroconversion (Fig. 1). Among 80 unvaccinated staff, interval infection was significantly higher among CNAs and nurses (aOR, 4.9; 95% CI, 1.4–20.7) than other staff, after adjusting for race and interval community incidence and facility infections. This risk persisted but was attenuated when utilizing the full study cohort including those with very recent vaccination (aOR, 1.8; 95% CI, 0.9–3.7). Conclusions: Midway through the first year of the pandemic, NH staff with close or common resident contact continued to be at increased risk for infection despite enhanced infection prevention efforts. Mitigation strategies, prior to vaccination, did not eliminate occupational risk for infection. Vaccine utilization is critical to eliminate occupational risk among frontline healthcare providers.
Funding: None
Disclosures: None

The impact of clinical risk conditions on influenza and pneumonia diagnoses in England: a nationally representative retrospective cohort study, 2010–2019
-
- Journal:
- Epidemiology & Infection / Volume 150 / 2022
- Published online by Cambridge University Press:
- 06 May 2022, e107
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Risk factors for severe acute respiratory coronavirus virus 2 (SARS-CoV-2) seropositivity among nursing home staff
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 28 October 2021, e35
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Our past creates our present: a brief overview of racism and colonialism in Western paleontology
-
- Journal:
- Paleobiology / Volume 48 / Issue 2 / May 2022
- Published online by Cambridge University Press:
- 19 August 2021, pp. 173-185
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Hidden in plain sight: the archaeological landscape of Mithaka Country, south-west Queensland
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Psychiatric Prescriber Attitudes, Experiences, and Proclivities Toward Digital Medicine and How They Influence Adoption of Digital Medicine Platforms
-
- Journal:
- CNS Spectrums / Volume 26 / Issue 2 / April 2021
- Published online by Cambridge University Press:
- 10 May 2021, pp. 144-145
-
- Article
-
- You have access
- Export citation
Complex multi-decadal ice dynamical change inland of marine-terminating glaciers on the Greenland Ice Sheet
-
- Journal:
- Journal of Glaciology / Volume 67 / Issue 265 / October 2021
- Published online by Cambridge University Press:
- 31 March 2021, pp. 833-846
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Aortic root aneurysm repair in a neonate with Loeys–Dietz syndrome
- Part of
-
- Journal:
- Cardiology in the Young / Volume 31 / Issue 5 / May 2021
- Published online by Cambridge University Press:
- 25 January 2021, pp. 848-850
-
- Article
- Export citation
5 - The Play at the End of the World
-
-
- Book:
- The Cambridge Companion to Theatre and Science
- Published online:
- 20 January 2021
- Print publication:
- 03 December 2020, pp 70-84
-
- Chapter
- Export citation
On the Ethics of Reconstructing Destroyed Cultural Heritage Monuments
-
- Journal:
- Journal of the American Philosophical Association / Volume 6 / Issue 4 / Winter 2020
- Published online by Cambridge University Press:
- 23 November 2020, pp. 483-501
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Utilizing a real-time discussion approach to improve the appropriateness of Clostridioides difficile testing and the potential unintended consequences of this strategy
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 10 / October 2020
- Published online by Cambridge University Press:
- 29 June 2020, pp. 1215-1218
- Print publication:
- October 2020
-
- Article
- Export citation
Search and recovery of aircraft parts in ice-sheet crevasse fields using airborne and in situ geophysical sensors
-
- Journal:
- Journal of Glaciology / Volume 66 / Issue 257 / June 2020
- Published online by Cambridge University Press:
- 24 April 2020, pp. 496-508
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Outcome of Conventional Bystander Cardiopulmonary Resuscitation in Cardiac Arrest Following Drowning
-
- Journal:
- Prehospital and Disaster Medicine / Volume 35 / Issue 2 / April 2020
- Published online by Cambridge University Press:
- 24 January 2020, pp. 141-147
- Print publication:
- April 2020
-
- Article
- Export citation
