


Introduction
Despite a general acknowledgement of their needs and slowly increasing inclusion, disabled people still experience significant and wide-ranging exclusion in most Western societies. These experiences negatively affect the day-to-day lives of disabled people and often constitute a reduction in their well-being. The majority of academic research on disability is, rightly, aimed at increasing the societal inclusion and positive lived experiences of disabled people; the initial societal response, however, was slow. Scholarly work on the phenomenon, originating in sociology and philosophy, has now rightfully become a multidisciplinary activity—the tendrils of which extend to ethics, political theory, political science, law, biology, sociology, anthropology, engineering, geography, architecture, history, archeology, medicine, economics, and beyond. The task of pulling these many and various perspectives together in an effort to create a consistent and cohesive theory of disability is, thus, a Daedalian endeavor.
The theoretical investigation of disability aims to construct a comprehensive definition or description of ‘disability’ from which ameliorative practical responses can be developed. The current hegemonic theories include the social and medical models—and, to a lesser extent, certain relational accounts such as the Nordic Relational Model. These models offer fundamentally different ontologies of the phenomenon of disability, and their criticism has been many and varied.Footnote 1 An overarching criticism of the hegemonic models is that, broadly speaking, they are unable to respond to the innate diversity of disabled people. This failure, I claim, is because the various approaches misinterpret disability as a sort of ‘thing’ rather than a ‘kind of experience.’Footnote 2
The picture theory of disability is a theoretical concept of disability, which shows how daily-living tasks or goal-like-ours are irremediably impeded by ‘picturing’ the experience of disability. The picture is then analysed, first linguistically, to show how and why a person in the picture experiences what they do, and then with an emotional focus to show how a person in the picture may be feeling. It is the perception of disability qua experience (and the phenomenological aspects of that experience) that differentiates the picture theory from both the hegemonic models and other relational accounts of disability. The result is a more comprehensive theory, which extends to all kinds of disabling experiences and which generates some unintuitive conclusions.
The Hegemonic Models
The initial theoretical approach to disability was clinical and arose largely out of necessity due to the return to work of amputee soldiers from the First World War.Footnote 3 This ‘medical model’ of disability became the de facto approach and not only offered a mechanism by which to treat disabled people but also guided policy formation in broader contexts such as welfare, distributive justice, and employment. The medical model largely reflects the ‘everyday’ concept of disability as a body with functional limitationsFootnote 4 , Footnote 5 and broadly interprets disability as a sort of ill-health. The most succinct presentation of the medical model comes from Christopher Boorse, who stipulates that health is “normal functioning, where the normality is statistical and the functions biological”Footnote 6; deviation from these biostatistical norms thus constitutes disease and “leads, at some stage, to disability.”Footnote 7 Disability for the medical model is, therefore, an individual condition and wholly a function of biostatistical difference.Footnote 8 This interpretation resulted in the much-criticized ‘medicalisation’ of disability, in which ‘fixing’ the disability became simply a matter of ‘fixing’ the individual.Footnote 9 , Footnote 10
Though the social consequences of impairment were being argued by Mildred Blaxter and others by 1976,Footnote 11 the social interpretation (or the British social model of disability) originated at a meeting between the Union of the Physically Impaired against Segregation and the Disability Alliance. A summary of the meeting, published as “The Fundamental Principles of Disability,”Footnote 12 drew concrete distinctions between disability and impairment: ‘disability’ was the disadvantage or restriction caused by the ableist expectations of society, while ‘impairment’ was simply the “lacking all or part of a limb, or having a defective limb, organism or mechanism of the body.”Footnote 13 The strong distinction between impairment and disability became the defining element of the British social model,Footnote 14 and the interpretation has become profoundly influential through authors such as Michael OliverFootnote 15 , Footnote 16 , Footnote 17 , Footnote 18 and Vic Finklestein.Footnote 19 , Footnote 20 , Footnote 21
Shifting disability from an ‘individual condition’ to ‘societally caused’ constituted both an ideological belief and a political tacticFootnote 22; the model was seen as the “‘big idea’ of the British disability movement,”Footnote 23 and its political formulation helped it to become a sort of litmus test for the disability rights movement. So armed, disability rights organisations were able to analyse policies, laws, and ideologies to determine whether they were sufficiently progressiveFootnote 24; the social model provided a benchmark from which to lobby if they were not.
Criticisms
The social and medical models are usually interpreted as standing in diametric opposition,Footnote 25 and by the mid-1990s, allegiances were wearing thin on both sides. Scholars began to criticise the British social model for excluding an individual’s personal experiences of impairmentFootnote 26 , Footnote 27 , Footnote 28 in the effort to divorce disabled people from “tragedy theory and victim-blaming explanations.”Footnote 29 Additionally, it became clear that the model had difficulty including people from certain groups, such as the Deaf community and people with mental health or intellectual difficulties.Footnote 30 , Footnote 31 By 2010, even the disability community’s fealty to the model had started to dwindle.Footnote 32 The model was not safe from theoretical criticism either: If the model’s categorical claim that ‘disability is caused by society’ were to be accepted, then the implication would be that all people with impairments are disabled and that all people with similar impairments are similarly disabledFootnote 33—a conclusion both false and misrepresentative. The model, once seen as a bastion of hope for disabled people,Footnote 34 has accordingly become recognised as logically problematic “both at the political level and the conceptual level.”Footnote 35
For its part, the medical model of disability was vilified by both academicsFootnote 36 , Footnote 37 , Footnote 38 , Footnote 39 , Footnote 40 , Footnote 41 , Footnote 42 and the disability rights movement.Footnote 43 , Footnote 44 In addition to its lack of social focus and for framing disability in terms of personal individual deficit, it is of little practical use in conditions where there is little to no ‘physical discrepancy,’ such as chronic fatigue syndrome, dyslexia, obsessive-compulsive disorder, and body integrity identity disorder. In part due to the difficulty the medical model has in responding to the growing list of mental disorders, and because medical practitioners were becoming more aware of the social and environmental factors relating to disability, the medical profession began to backpedal from their individual-deficit account.Footnote 45 By 2007, the Institute of Medicine’sFootnote 46 Committee on Disability no longer incorporated “ideas and values associated with the medical model,”Footnote 47 and instead acknowledged the “growing recognition that disability is not inherent in individuals, but rather is the result of interactions between people and their physical and social environments.”Footnote 48 This shift in recognition mirrored theoretical approaches that recognised the importance of both the individual and the environment—approaches which became broadly understood as ‘relational accounts.’
The Disability Theory Continuum and the Relational Approach
The social and medical models can be interpreted as lying at each end of a continuum, represented in Figure 1. The British social model is shown on the left, and the medical model on the right. The space in between is occupied by the various relational accounts of disability, which interpret the relation between a disabled person and their environment to be the cause of disability. While the locution ‘relational concept’ or ‘relational approach’ is used globally, the Nordic countries (which are less directed by the political agenda of the disability rights movement)Footnote 49 refer to the idea as the ‘environmental turn.’Footnote 50 , Footnote 51

Figure 1 The disability continuum.
The environmental connection originates in Bengt Nirje’s ‘Normalisation Principle,’Footnote 52 , Footnote 53 which maintains that the lives of the mentally impairedFootnote 54 could (and ought) be normalised to more reflect the lives of everyone else. At the time he was writing, mentally impaired people were largely institutionalised and forced to live homogeneous and isolated lives; Nirje argued that normalisations like replicating the distinction between work and home time, altering routines, and varying an individual’s surroundings would help provide a better quality of life. The relationship between a person’s abilities and the functional demands of the environment coalesced in Scandinavia and Europe to the ‘Nordic Relational Model of Disability’Footnote 55 and can be characterised as an empirically sensitive, multi-level approach that is both relative and interactionist.Footnote 56
Several years before Mårten Söder coined the developing Nordic approach ‘the relative perspective’ in 1999,Footnote 57 the relational (qua environmental) element of disability was discussed by non-Nordic authors such as Ron Amundson. Amundson initially believed that “the property of having a particular [impairment] is an attribute of a particular person”—but the property of being disabled is relational.Footnote 58 By the time Amundson seceded the relational aspect of disability and nailed to his mast the colours of the British social model,Footnote 59 , Footnote 60 relational accounts had become more heavily debated. These accounts included amongst their number Julian Savulescu and Guy Kahane’s ‘welfarist account’Footnote 61 and the ‘bio-psychosocial model.’Footnote 62
Relational approaches, however, are not free from criticism: Thomas Shakespeare cautions that the British social model already describes the “relationship between people with impairment and a discriminatory society”Footnote 63—and that a proper reading of the British social model would be that “disability itself is caused solely by the environment.”Footnote 64 Taking a different approach, Lennard Nordenfelt worries that relational interpretations (at least at the time he was writing) did not properly consider the importance of an agent’s goals.Footnote 65 For Nordenfelt, disability is a species of inability that “should be related to the individual’s own vital goals.”Footnote 66 Nor was Nordenfelt alone in recognising the importance of goal achievement: Amundson, in his relational epoch, also claimed that people are disabled “only with respect to a particular environment and a particular goal.”Footnote 67 I agree with both Nordenfelt and Amundson on the importance of goal accomplishment; thus, whether or not one can meet one’s daily-living tasks or ‘goals-like-ours’ constitutes a necessary part of the picture theory of disability’s formulation.
A Model Difficulty
The failure of the disability continuum to adequately respond to the phenomenon of disability can be shown by considering Brett Nielsen. An image of Nielsen, shown in Figure 2, playing the piano is taken from the documentary Brett: A Life with No Arms. Footnote 68 The documentary shows, amongst other things, Nielsen playing the piano with his feet; Nielsen does not identify as disabled.Footnote 69

Figure 2 Brett Nielsen playing the piano with his feet. A still from Graef R, Nielsen B. Brett: A Life with No Arms. Documentary, London: BBC; 2015:59 min., colour.
Nielsen’s experiences in life as a person with no arms seems inconsistent with hegemonic analyses of his case: The medical model of disability views Nielsen as disabled simply because he has no arms—an easily quantifiable deviation from biostatistical norm. The social model’s dogmatic approach to ableist social discrimination similarly identifies Nielsen as disabled because the design of the built environment (including pianos) necessarily oppresses those without arms.Footnote 70 Relational models fair no better than the hegemonic medical and social models, and collapse (as Shakespeare pointed out) into a sort of social model analysis—the ‘mismatch’ between Nielsen and the built environment is a result of the built environment being designed for people with arms and Nielsen not having any.
Indeed, our everyday intuitions about disability fair little better: We naturally assume that someone without arms must be disabled. Yet when Nielsen is observed in and about his daily activities, such as rolling a cigarette (Figures 6 & 7) or shopping for cheese, the difficulty and frustration normally associated with disability is not evident (neither in his actions nor in his emotional responses to daily activities). So, if the hegemonic theories of, and our everyday intuitions about, disability seem to conflict with Nielsen’s own lived experience, is there some other way to interpret disability? The answer, I think, is yes—but it requires a fundamental shift in the way disability is understood.
The Picture Theory of Disability
Models on the disability continuum seek to identify a specific thing (or set of things) as the location qua cause of ‘disability’ -- yet, these approaches seem to conflict with diverse perspectives on disability, such as Brett Nielsen’s.Footnote 71 I believe the overall difficulty with (and cardinal reason that) the various approaches that fail to generate a successful account of disability is because they make a category error.
Homer Rutledge created the image shown in Figure 3 as an exercise for non-dyslexic people to “better understand the difficulties and frustrations a dyslexic person faces even when trying to read something as simple as a poem.”Footnote 72 While the image is not a literal representation of dyslexia, what it generates in the average reader is a kind of difficulty—an impediment—in reading the poem. The category error made by the disability continuum models, then, is that disability is a kind of thing when, in fact, it is a certain kind of experience: One does not have a disability, one experiences disability. Nounal accounts of disability fail because the experience of disability is an aspect of ‘doing’ rather than ‘something’; it confuses locating ‘disability’ with locating ‘hurriedly.’Footnote 73

Figure 3 A dyslexic poster by Homer Rutledge. Source: behance.net [cited 2022 Nov 2]. Available at https://www.behance.net/gallery/2252974/Dyslexia-Poster (last accessed 14th Feb 2023).
In natural languages, verbs describe doings; however, verbs only indicate what action is being done: throwing, climbing, walking, reading. To know in what way that action is being done, the verb must be modified by an adverb: the ball is thrown awkwardly; the stairs are climbed easily; she walked painfully; they read frustratedly. If attention is paid to the manner in which verbs are modified, then it is possible to know if and how an action is being blocked for a particular person in a particular circumstance. To talk of disability as a ‘verbal’ concept would be unhelpful—instead, the experience of disability should be understood as an adverbial concept.Footnote 74
Instead of naming who is or is not disabled (and by what), the picture theory of disability is concerned with identifying if, how, and under what conditions a person experiences disability. There are two elements or analyses required to build a picture theory of disability:
Element 1: The picture—shows us how and why people in the picture experience what they do.
-
• Metaphysically grounds the theory,
-
• Includes additional support material (a Q&A, testimony, or similar),
-
• ‘Pictures’ a situation, which permits an
-
• Analysis of the adverbial and adjectival modification of the action.
Element 2: Naive sympathetic conversion—shows us how a person in the picture is feeling.
-
• Develops an empathic analysis of the emotional effect of the action in the ‘picture,’ which is then used to determine:
-
• Whether how a person feels in an action is appropriate for the activity, and
-
• Whether an observer becomes motivated to intercede to reduce frustration (conation).
The ‘Picture’
Roughly construed, the ‘picture’ is a mechanism “through which it is possible to ‘unpack’ the meaning of disability for the person experiencing it.”Footnote 75 While images or videos can be part of the process, the ‘picture’ in the picture theory of disability does not refer to the images themselves, and instead is named for the process of imagining—or ‘picturing’—the world in a way that accurately represents the way it is. Essentially, the picture theory of disability holds that the experience of disability can be understood by simply observing or ‘picturing’ those occasions in which it is said to occur.
The formative analysis can begin with any sufficiently detailed representation of an activity that accurately portrays the experience of disability and which documents the relevant relations between agents and objects in the world. The representations can include images, video footage, a written transcript,Footnote 76 in-person observation, and so on; however, the medium must capture both the adverbial nature and the emotional aspects of the activity. The experience of disability is particular because each individual adapts uniquely to the world, so a representation of that activity must reflect or portray the experiences of that given individual. The resultant analysis, therefore, will be particularist, and the analysis of the experience of disability for one person will not necessarily extend to another individual (even if their impairments are similar).
The purpose of formative analysis is to identify the constituent objects and relations in the picture—a process similar to that which Ludwig Wittgenstein employed in his picture theory of language. Wittgenstein sought to delineate the relationship between a proposition, a state of affairs, an object,Footnote 77 and a complex.Footnote 78 Propositions that ‘picture’ the world, he thought, can represent it either truly or falsely; “if a fact is to be a picture, it must have something in common with what [the picture] depicts.”Footnote 79 Thus, the proposition ‘the cat in the box is alive’ is true if and only if the objects and relations in the proposition properly map those in reality—that is, there exists a box with a cat in it, and the cat is alive.Footnote 80 Wittgenstein ultimately dropped his picture theory of language, but the ‘picture’ framework is useful to the picture theory of disability both as a means of metaphysically tying the experience of the activity to the activity itself and in delineating the elements or objects relevant to the experience of disability.
Objects in the picture theory of disability are considered at a much broader level than were necessary for Wittgenstein; a careful explication of exactly what constitutes a ‘wheelchair,’ therefore, is not necessary—it is enough that ‘wheelchairyness’ is understood and that a wheelchair-like thing can be picked out from the picture. The final level of object analysis is reached when the list of objects in a picture shows us all the elements related to a given activity. An analysis of the image shown in Figure 4, for instance, would include a person wearing a coat, a bag, flat sandy ground, mountains, a barn, hip-height rocks, light cloud, and birds.

Figure 4 The war doctor carrying a sack. A still from Steven M. Doctor Who; The Day of the Doctor. Film, London: BBC; 2013.
In addition to breaking apart the image into its various elements, the ‘formative analysis’ requires that the relations between objects are also analysed; they are interpreted as verbal and positional propositions such as ‘a person is stood holding the bag over their right shoulder,’ ‘the barn is in front of the person,’ and ‘the barn is closer to the person than the mountains.’ In order to do more work, however, this holistic or formative analysis needs to be fleshed out, and it is here that the colour—the adverbial/adjective modification and the goal of the activity—can be added by an observer to describe the way the action(s) in the picture are being performed. This ‘colour analysis’ is performed by reflecting both on the picture and on the support material. With this adverbial and adjectival modification added, the analysis may look something like ‘the heavy bag is borne with effort over the right shoulder by an old, but able-bodied, person,’ ‘the barn is a relatively long walk in front of the person,’ and so on.
The support material (providing the lived experience context) can be sourced through a question-and-answer session or general discussion and should seek to target both the needs and the goals behind the activity and the physical experience of performing the action or activity. Information about the emotional aspects of the activity can also be collected at this stage, though those data are analysed separately through Naive Sympathetic Conversion (described in the next section). The support material data relate the intended purpose and importance of the activity to the observer and can include content such as how often the activity is performed, whether the activity is related to work or pleasure, and whether the goal was ultimately achieved. The primacy of the lived experience is paramount, as tasks performed by disabled people may appear awkward or unusual to able-bodied persons but are not necessarily perceived as such by the individual.
The complete holistic analysis, ultimately, should contain all the information necessary to generate a complete ‘picture’ of the experience and can be thought of as preparing a transcript of the activity such that the action could be recreated as a scene from a play. The image in Figure 4 is a screenshot taken from the film “The Day of the Doctor”Footnote 81; an analysis made of the scene in the film might look something like this:
The old man was tired and carried the heavy bag over his right shoulder with some effort—the bag needed constant adjustment to ease the discomfort it caused in the bearer’s back and right shoulder. The ground was flat, but the soft sand made walking difficult and he paused regularly due to fatigue. He only needed to carry the bag to the barn and not to the mountains (which would have been a much farther journey), and he was thankful that the task would soon be completed. The bag contained a machine that would end the Time War; the task of setting it, was, literally, a matter of life and death and of the upmost importance to the old man.
The above analysis contains all of the information required to determine whether the pictured activity resulted in the experience of disability. In the example, though the activity was tiring, hard work, and important, it did not result in the experience of disability because the adverbs and adjectives describing the activity were not negatively modified to the extent that the goal was irremediably impeded, nor was the effort involved in carrying the sack beyond the individual’s capacity for such an activity. Once the holistic analysis is complete, it can then be synthesised with Element 2: Naive Sympathetic Conversion to determine the emotional experience of the action or activity.
Naive Sympathetic Conversion
The adverbial analysis of a picture has some analytic limits: It is only able to show us if, when, where, in what way, and to what extent an impediment to an action is occurring—it does not tell us whether the effect of the activity or action is emotionally excessive, unremitting, or otherwise problematic. In order to determine such information, an additional analysis is needed to help understand how it feels to perform a certain action in a certain way.
Humans are able to interpret a tremendous amount of information from slight changes in body language and expression—particularly those that carry emotion. David Hume argues that this connection is strong enough that we are able to share in the ‘passion’ (what we might now call ‘the emotional sentiment’) of another simply by observing themFootnote 82: A person’s passions, pains, and pleasures “strike upon us in a lively manner, and produce an emotion similar to the original.”Footnote 83 The amount of emotional information that can be communicated by an image can be shown through Figure 5, which shows Laith Majid, a Syrian refugee, holding his son and daughter as they land on the island of Kos in 2015.Footnote 84 The image is a candid and powerful shot, but it is evocative because the emotions that Majid was feeling are imminent and communicable; they are, thus, readily interpreted and shared by the viewer.

Figure 5 Etter D. Laith Majid, a Syrian refugee, holding his son and daughter, arrives on the Greek island of Kos; 2015 Aug 15. The Guardian. 2015 Sept 8; Syrian man pictured crying as his family landed in Greece finds refuge in Germany.
The neurobiological process that makes us share in the feelings of others (what Hume calls a ‘sympathetic conversion’Footnote 85 and what is now known as ‘self-other conjoining’Footnote 86) is a sort of “resonating of the protagonist’s mental and emotional states with that of someone else.”Footnote 87 The description of the process by Christian Keysers is strikingly similar to Hume’s: “Our brain first simulates what the other person’s face is doing in the premotor cortex, and once you share the facial expression in your premotor cortex, your [insular cortex] kicks in, making you share the feelings of that person.”Footnote 88 The activities in the prefrontal cortex not only replicate in our minds an action performed by another, but they also contribute to the ‘cognitive’ aspects of empathy, such as “taking someone else’s perspective and vicariously identifying with it.”Footnote 89
The brain’s capacity to mirror can also have a strong effect on us when we watch somebody do something: Watching someone type slowly with one finger, for instance, can lead faster typists to feel frustrated and impatient, and cause them to want to take over the typing. This sensation occurs because when an action is replicated in the observer’s brain, it is reproduced at the observer’s skill level (which may be quicker if the observer happens to be a better typist). The mismatch between how the watched action is performed and how the action is replicated in the observer’s brain (perhaps at a different speed or with greater success) can generate a powerful impetus to intercede or take over the task to reduce both the difficulty of the task for the individual and the frustration felt by the observer.Footnote 90 The motivation to intercede—which I call ‘conation’—is useful during the synthesis of the theory, as it is a strong (but not categorical) indicator that a disabling experience may be occurring.
The Synthesis
To show how the various parts of the analysis are pieced together, a hypothetical situation similar to the one shown in Figure 4 is required. Acknowledging that the scenario below cannot replicate the level of detail or context that would be available from a video clip or a real-world example (nor can it offer a treatment of the various ‘what ifs’ that can be laid against such a simplistic example), and to aid the understanding of the process, the scene below is intentionally austere: ‘A set of stairs into a high-rise office building in some random Western city and an individual seeking entrance to the building.’ From this simplistic hypothetical scenario, and depending upon the relevant elements in the picture, we might generate two possible pictures:
Picture 1

Picture 2

The two pictures differ in that the target individual in Picture 2 is a wheelchair user, otherwise the elements of both pictures are similar. The next step is to perform a colour analysis on the scene. To do this, let’s assume that the hypothetical video clip of the scene shows the experience of the target individuals and that the supplementary material includes a question-and-answer session containing the following information:
-
• The target individual is going for a job interview,
-
• The stairs are external to the building and there is no other way to get in the building without stairs or the use of the delivery loading bay ramp in the basement,
-
• There are people hastily running up and down the stairs to get out of the weather, and
-
• That the target individual in question has not had many job interviews in the past and is a suitable candidate for the position.
From the additional information, we can build two full analyses, as shown in Table 1.
Table 1. A Picture Theory Analysis of Two Scenarios
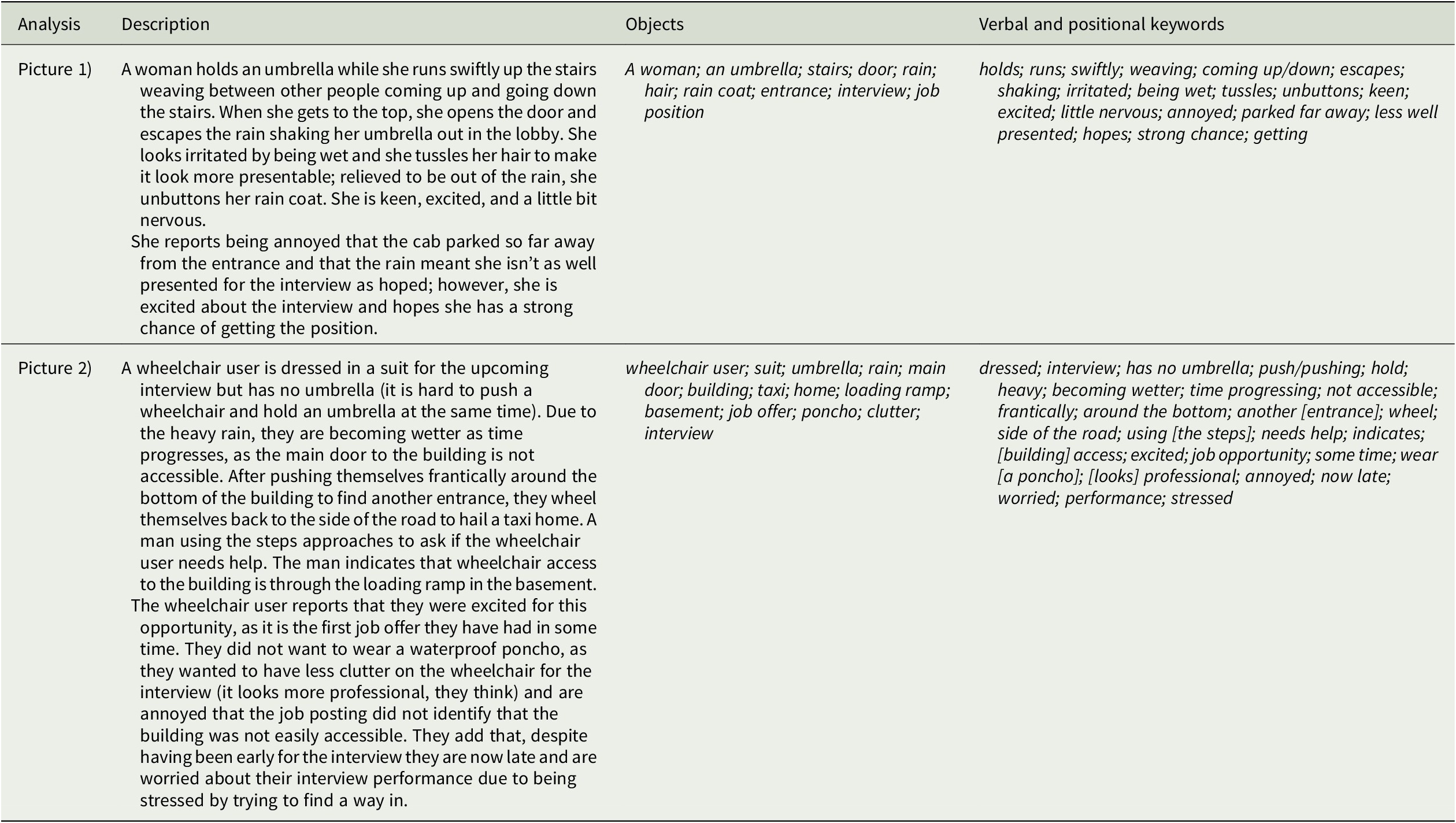
Despite the emotional states of our would-be interviewees being somewhat lost due to the lack of an actual video of the scenario, it is still clear that (1) the wheelchair user was worried, was annoyed, and nearly gave up on the interview; and (2) the lady with the umbrella was irritated, nervous, and excited. That someone on the stairs tried to help the wheelchair user find an alternative way into the building demonstrates that there was a recognition that the wheelchair user was not achieving some goal and they felt a need to intercede.Footnote 91 In short, the physical and emotional effects of this specific situation differ from those of the other interviewee in that they nearly constituted an unremitting irremediable difficulty, frustration, or complete impediment in the conduct of a specific daily-living task or goal that is engendered by a specific relationship between a person and their environment. Footnote 92
The picture analysis shows how the experience of disability does or does not occur: Words in the analysis of Picture 1, such as ‘swiftly’ and ‘relieved,’ can be contrasted with words in Picture 2, such as ‘frantically’ and ‘annoyed.’ In addition, while the person in Picture 1 was drying off inside the building before her interview, the wheelchair user in Picture 2 was heading away from the building to hail a cab—intimating that the goal was, at least initially, unattainable and making the interview required the help of others. Though the naive sympathetic conversion analysis is limited due to the brevity of the scripted scene, it was still able to show if, when, and where negative emotions were generated by the experiences (and in what way and to what extent they were shared by the observer and others).
An individual’s own phenomenologicalFootnote 93 perspective is provided through supplementary material (a more discursive and extensive version than above); the words used to describe their experience of the situation can be compared with the observer’s to balance the observed perspective with the lived experience. The negative modification of words is an indicator that the individual may have experienced disability; contrarily, if the modification of the verbs and adjectives is positive, then there is likely no experience of disability. In the above scenario, the wheelchair user was not fully prevented from achieving their goal, but there was a clear impediment to it, which negatively affected their experience and which would not have been resolved by shifting aspects of the scenario such as changing the date of the interview.
These analyses can indicate a disabling experience to a greater or lesser extent, depending upon the strength of the material and the resulting picture. Similarly, conation, in and of itself, is not sufficient to identify disabling experiences, as the motivation to intercede can also occur when we see able-bodied people struggle with an activity such as changing a tire on a car or carrying heavy bags. However, together with the linguistic and situational analyses, conation can be a helpful indicator that there is something wrong with the picture; and, because of the proclivity for problem-solving, when conation does appear, it often targets the exact nature of the difficulty and naturally reveals novel ways to reduce the negative experiences. It is in this way that conation can be used to supplement or drive normative applications of the picture theory of disability.
The Distinction Between Disability and Difficulty
The nature of ‘capacity’—the innate ability for someone to perform a certain task or achieve a certain goal—is challenging to delineate without deferring to the medical model of ‘species-typical norms.’ Indeed, trying to define what constitutes ‘normal functioning’ is, in and of itself, complicated given that not all able-bodied individuals can achieve the same kinds of performance. I would, for instance, be unable to climb the Phoenician steps at Capri; any ‘picture’ of such an attempt would include my ruddy face, wheezing disposition, and exclamations of maleficence. An observer might conclude that I was experiencing a significant impediment to climb—and they would be, to a certain extent, right. The Phoenician steps are a well-understood challenge for many able-bodied people and, unless an individual has a remarkable capacity for such activity, the physical exertion of the climb is generally quite unpleasant. However, the climb does not really constitute an ‘unremitting or irremediable experience’: Once the climb is made (or balked), or were I to spend years increasing my cardio capacity (and, perhaps, step away from the sour cola bottles), then the steps might be climbable without the level of frustration that many other people exhibit.
Yet there is an obviousness to the way in which activities are challenging for people who experience disability and for those who do not. The experience of disability constitutes an unremitting, irremediable difficulty, frustration, or complete impediment to some action or activity—this time and every time. Furthermore, the kinds of scenarios that generate the experience of disability do not, generally, become easier or less challenging if the target individual increases their capacity for climbing stairs, for instance. Furthermore, the activity must be one which the individual themselves considers problematic and which is not, broadly constituted, simply difficult—I, like many people, recognize the Phoenician steps as a significant physical challenge, but brushing my teeth is not. Consequently, disability might be experienced if individuals are unable to brush their teeth or leave their house, whereas diving for Tahitian pearls is beyond the capacity of most humans because it is, ordinarily, immensely challenging.
To help determine the extent of what is ‘ordinarily’ challenging, the picture theory’s analysis depends upon both a phenomenological representation and (a more objective) third-party interpretation. Despite their objectivity, observers must work to actively consider the experience itself, and not let their ‘everyday’ intuitions of disability sway or bias the analysis. While an observer might anticipate that Brett Nielsen would experience certain frustrations to daily living such as rolling a cigarette, for example, Nielsen’s lived experience helps circle what is or is not within the capacity of the individual. While Nielsen can roll his own cigarettes (Figures 6 and 7), that capacity should not become a standard to which all people without arms are held; it is the primacy of the lived experience within the picture theory of disability that helps avoid the kinds of normalized capacities that have encumbered the social and medical models.

Figure 6 Brett Nielsen rolling a cigarette with his feet. A still from Graef R, Nielsen B. Brett: A Life with No Arms. Documentary, London: BBC; 2015:59 min., colour.

Figure 7 Brett Nielsen rolling a cigarette with his feet
Savulescu and Kahane rightly observe that what makes ‘disability’ morally relevant is that it is (generally) correlated with a reduction in well-being.Footnote 94 However, as the social model correctly points out, there is an important difference between a ‘bodily or intellectual difference’ and ‘disability’: Just because a person has a difference does not mean that that person is disabled. People with chronic fatigue syndrome experience extended periods of profound fatigue, dizziness, and difficulty focusing. The experiences of weakness or lack of concentration are imminently disabling and can extend for months at a time—but those individuals may also experience periods in which they experience little to no impediment to their tasks or goals. In such a situation, the ‘irremediability’ can be said to extend both to the incurability of the condition itself and also to the way in which the symptoms, when they occur, frustrate daily-living tasks and goals-like-ours.
The phenomenological perspective of the experience of disability is, therefore, crucial to identifying the distinction between what is difficult and what is irremediably frustrated. If an individual claims to be experiencing disability in a given activity, and an analysis on the activity shows negative modification of the verbs, then the person is likely experiencing disability—regardless of whether that activity ‘looks’ difficult or easy to the observer.
Improving on the Hegemonic Models
The picture theory of disability improves on the hegemonic models in a number of ways. Firstly, the political aspect of the social model is eliminated, permitting improvements to be targeted properly on the experience of disability. This unfettered analysis distances society from the blame of causing disability without also removing the obligation to improve the well-being of disabled people. Secondly, the theory is able to identify occasions in which the experience of disability intrudes upon either the well-being or the goal achievement of an individual—this includes people with mental conditions or impairments (cases which often flounder other models). Thirdly, it grants agency to the individual, expunges the ‘individual-deficit’ discourse, and frees society from the bootstrapping problem of identifying prejudiced design and policy. Fourthly, it offers a mechanism to resolve the experience of disability from the ground up (analyses could be conducted, for example, as much by human resource department personnel as it could by healthcare specialists). As a result, change can happen at much lower levels where the experiences are most imminent and can be focused to resolve specific barriers for specific individuals. Fifthly, because the analysis is particularist, it is not constrained to only generate broad-spectrum ameliorationsFootnote 95; for persons with broadly similar impairments, the picture theory permits the resolution to be tailored to the individual.
Perhaps, however, the most notable improvement is that the picture theory of disability looks beyond the individual and the environment to the frustration of the action—focusing on that element of the experience of disability that makes it problematic. Regarding the office interview scenario presented above, the various approaches seek to identify causes of disability: The social model holds that the non-inclusive design of stairs is responsible. Yet there is nothing per se disabling about stairs—most people use stairs without difficulty (including Chris Koch, Figure 8). The medical model argues that an individual’s lack of functionality is responsible, but some peoples’ bodily differences do not affect the achievement of their daily-living tasks or goals-like-ours.

Figure 8 Chris Koch climbing stairs. A still from YouTube. Talks at Google: Chris Koch: “If I Can ….” 2015 Sept 3 [cited 2015 Sept 4]. Available at https://www.youtube.com/watch?v=RvQzJIB8Sn0 (last accessed 11th Feb 2023).
Relational accounts improve somewhat on the two hegemonic models. They are able to account for people like Chris Koch, and for why old and infirm people can find stairs challenging. However, the relational models constitute a broad approach, rather than any distinct theory or tool. The Nordic ‘relativist interactionist perspective,’ for instance (likely the most cohesive and well-structured of the relational approach), is not a theory at all and, at best, requires several levels of analysis from multiple methods and approaches. Savulescu and Kahane’s welfarist account fares a little better: While it offers a clearer and more cohesive mechanism for defining disability than the Nordic approach, it ultimately depends upon “the empirical facts plus whatever is the true account of wellbeing.”Footnote 96 Thus, the successful application of the account hinges upon first determining “the nature of ‘good’”—a trivial matter of practical philosophy which, despite 2,500 years of debate, somehow remains unresolved.
Though the picture theory of disability, technically, could be considered a species of relational account, its focus is on the experience qua disability not the relationship qua disability. It is, therefore, importantly distinct from other relational accounts and does not reside on the same disability continuum. Application of the picture theory tends to provide less intuitive results, but which more accurately and consistently represent the lived experiences of disabled people. If an individual were unable to maintain a job because of difficulty leaving the house without repeatedly checking that the stove is off or the door is locked, then that person experiences disability. However, if it were to analyse Brett Nielsen rolling a cigarette or driving a JCB, then it would identify no experience of disability.
Conclusion
The picture theory of disability provides a particularist account of disability that holds there is no such thing as being disabled—rather, there are certain people who have disabling experiences. The theory technically constitutes a subspecies of relational approach, as the relationship between individuals and their environment is important in the formulation of the picture. However, the focus on the experience of disability rather than the existence of disability sufficiently differentiates it from the hegemonic models and other relational accounts of disability.
The theory improves in many ways on the current models of disability: by identifying the exact ontology of an irremediable impediment to a daily-living task or goal-like-ours, by extending to those with mental impairments and learning difficulties as well as those with physical impairments, by providing agency to the individual in the analysis of their lived experiences, and by removing from the experience any blame or responsibility. Additionally, the picture theory’s formulation permits it to also operate as both a metric and heuristic by which policies, procedures, and design can be evaluated from the ground up.
The picture theory of disability introduces the concept of ‘conation’ as the motivation felt in an observer to act or intercede in an effort to reduce a frustrating or overbearing experience. Conation can be employed to develop new responses to the experience of disability, because it naturally focuses on eliminating or working around the element in a situation that results in an action being blocked for a particular individual.
Finally, the picture theory of disability constitutes a novel, phenomenological, particularist, and purely descriptive model of disability that makes no normative claims and broadly defines the experience of disability as “an unremitting irremediable difficulty, frustration, or complete impediment in the conduct of a specific daily-living task or goal that is engendered by a specific relationship between a person and their environment.” The theory’s shift in focus allows new ways of responding to the experiences of disability to ‘fall out’ of the analyses and provides a structured process from which broader healthcare and social policies can be designed and evaluated.
Competing Interest
The author declares none.









