



Background
Epidemiological research has shown that men are at increased risk of several different infectious diseases [Reference Washburn, Medearis and Childs1]. However, data addressing the underlying biological mechanisms are scarce. Staphylococcus aureus (S. aureus) is more frequent in men compared to women, both as a nasal coloniser and as a causative infectious agent [Reference Olsen2, Reference Benfield3]. Nasal colonisation is a major risk factor for S. aureus infection [Reference Bode4]. Thus, the identification of biological pathways underlying sex differences in nasal colonisation is important not only to enable a better understanding of host factors in colonisation but also to enable the development of preventive interventions that take sex differences into account.
It is well known that immune functions differ by sex and age [Reference Klein and Flanagan5, Reference Simon, Hollander and McMichael6]. Sex-steroids are key regulators of both the innate and adaptive immune system, and hormone levels and actions are context (i.e. sex and age) dependent. Recently, we showed for the first time that higher levels of circulating testosterone in adult women [Reference Stensen7] and use of progestin-only contraceptives (structurally related to testosterone) in younger women [Reference Stensen8] are associated with lower prevalence of S. aureus nasal carriage. To our knowledge, no epidemiological study has examined whether endogenous sex-hormone levels are associated with S. aureus nasal carriage among men.
Thus, the aim of this study was to examine possible associations between endogenous sex-steroids and S. aureus nasal carriage in a large male population sample.
Methods
We used data from male participants in the population-based Tromsø6 study (2007–2008), North Norway, 66% attendance. The study included measurement of height and weight, blood samples and interview and questionnaire on lifestyle and health. Trained nurses at the 6th Tromsø Study screening centre collected nasal swab samples from 1741 male participants. Each nasal vestibule was sampled with the same NaCl (0.9%)-moistened sterile rayon-tipped swab which was rotated three times. The swabs were immediately placed in transport medium (Amies Copan, Brescia, Italy) and stored at 4 °C for a maximum of 3 days. Personnel at the Department of Microbiology and Infection Control, University Hospital of North Norway, (UNN) Tromsø analysed the microbiological samples. The specimens were cultured on blood agar (Oxoid, UK) for growth control and chromID-plates (SAID) for S. aureus detection (bioMérieux, Marcy I'Etoile, France). The agar plates were incubated for 42–48 h at 37 °C. To retain high specificity, colony morphology was examined, and the most dominating colony type on the SAID plate was confirmed as S. aureus by the Staphaurex plus agglutination test (Murex Diagnostic Ltd, Dartford, UK). Growth of any bacterial colonies on agar plates was registered as a valid culture. A second set of nasal swabs was collected with a median interval of 28 days.
Among the 1741 male participants that provided a nasal swab sample, serum concentrations of sex-steroids were measured in 888 individuals (because of limited funding and additional consent for blood sampling). After exclusion of 19 individuals taking antibiotics the last 24 h and 117 individuals with only one nasal sample, 752 men were included in the present analysis.
Liquid chromatography tandem mass spectrometry (LCMS/MS) was used to measure serum concentrations of testosterone, androstenedione, 17α-hydroxyprogesterone (17-OH progesterone) and progesterone [Reference Stensen7]. Serum concentrations of gonadotropins (luteinising hormone (LH) and follicle-stimulating hormone (FSH), binding proteins (sex-hormone binding globulin (SHBG) and albumin)), dehydroepiandrostenedione sulphate (DHEAS) and 25-hydroxyvitamin D were assessed by immunoassay methods. Estimation of bioavailable testosterone (free and albumin-bound testosterone) was performed using the equation ‘(testosterone/SHBG) × 10’ [Reference Channer and Jones9].
Statistical analyses were performed using Stata/MP 15.1 for Macintosh, with significance level set to P < 0.05. Univariable associations were assessed by χ 2 test, Student's t test, or Mann–Whitney U test. Multivariable logistic regression models were fitted to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for S. aureus persistent nasal carriage by change in sex-steroid concentrations, while adjusting for potential confounders. A sensitivity analysis on an age-stratified population (cut-off 55 years, median age) was performed, as both concentration of serum androgens and S. aureus persistent nasal carriage were inversely related to age. DAGitty 3.0 was used for model selection, and possible interactions were assessed for in the final model.
Results
Among the 752 males, age 31–87 years, the prevalence of S. aureus persistent nasal carriage was 32%. Persistent nasal carriers were younger, had lower vitamin D levels and lower prevalence of current smoking than others (intermittent or non-carriers; results not shown).
We found no association between any circulating sex-steroid and S. aureus nasal carriage in the total population when adjusting for age and body mass index (BMI) in a multivariable logistic regression model (Table 1).
Table 1. Associations between hormonal status and S. aureus persistent nasal carriage in men

Adjusted odds ratios (OR) and 95% confidence intervals (95% CI) of carriage by one unit increase in serum hormone biomarkers The Tromsø6 study, n = 752.
a Persistent nasal carriage: two S. aureus culture positive nasal swab samples.
b Adjusted for age and body mass index (BMI) in multivariable logistic regression analysis.
Among men aged 55 and above, persistent nasal carriers had lower mean serum concentration of both testosterone and SHBG compared to others (P = 0.028 and 0.052, respectively, Table 2). Men aged 55 and above had lower odds of persistent nasal carriage with lower concentration of testosterone (OR = 0.94 per nmol/l change in testosterone; 95% CI = 0.90–0.98). When adjusting for BMI, the OR for persistent nasal carriage was 0.96 (95% CI = 0.91–1.01) per nmol/l increase in testosterone in the oldest age group (result not shown).
Table 2. Serum concentrations of sex-steroids, gonadotropins and binding proteins by S. aureus nasal carrier state

Age group (median split) in men. Data are presented as mean (s.d.). The Tromsø6 study.
s.d., standard deviation.
a Number may vary due to missing values.
b Others; Intermittent carriers (one positive nasal samples of two samples in total) or non-carriers (two negative nasal samples of two samples in total).
c Mann–Witney U test.
d Calculated by the equation ‘(testosterone/SHBG) × 10’.
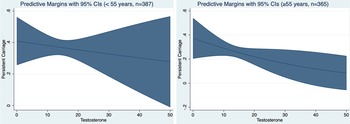
There was an inverse dose-response relationship between serum testosterone concentration and S. aureus persistent carriage. The dose-response relationship was most evident among men aged 55 and above (Fig. 1).

Fig. 1. Probability of S. aureus persistent nasal carriage according to serum testosterone concentration ((nmol/l), range 0.4–44.3). The Tromsø6 study, male participants.
Discussion
In a recent study among women in the Tromsø6 study, we showed that higher levels of testosterone and bioavailable testosterone were associated with lower prevalence of S. aureus nasal carriage [Reference Stensen7]. In the present study of the male population, we found no statistically significant associations of sex-steroids, gonadotropins and binding-proteins with the prevalence of S. aureus carriage when adjusting for BMI and age. In the age-stratified sensitivity analysis, we found an inverse association for testosterone among the oldest group (≥55 years).
In our population-based data, there was a strong inverse association between age and serum testosterone (results not presented), that is consistent with the described progressive decline in testosterone levels in healthy men between 25 and 75 years [Reference Svartberg10]. The decline in prevalence of S. aureus nasal carriage across adulthood is well known [Reference Sangvik11]. Both age-related changes in testosterone and bacterial flora may be adaptations to ageing, but the contribution of ageing per se vs. lifestyle/nutrition and comorbidities (i.e. confounding factors) to these changes is not clear. Importantly, when adjusting for both age and BMI in our analysis, we found no statistically significant associations between sex-steroid concentrations and S. aureus nasal carriage. Thus, we cannot conclude that testosterone is a predictor for S. aureus nasal carriage in men.
In this study, we collected only one venous blood sample for analysis of sex-steroid hormones. Male sex-steroid hormones are diurnal, but less so compared to women and this may result in a more representative value with only one measurement. Testosterone in men has a circadian rhythm with optimal sampling from 8 to 10 am. In our study, the blood samples were taken from 8 am to 8 pm, thus attenuating a potential underlying population effect through non-random measurement bias towards the null. Studies have shown that the circadian rhythm is lost in elder men [Reference Bremner, Vitiello and Prinz12], and we believe that the stratified model of men over 55 years of age better represent the true underlying population effect.
We are not able to conclude from our data that circulating sex-steroid concentrations are related to S. aureus nasal carriage in men. This is in contrast to our recent findings in women [Reference Stensen7], and may represent, among others, imprecision in measurements, a too broad age range, or a different relationship between sex-steroids and immunity in men and women. The role of endogenous sex-steroids in S. aureus colonisation should be addressed in future prospective studies. Future studies will benefit on including a larger study size and standardised measurements on sex-steroids.
Acknowledgements
We thank each participant in the sixth Tromsø Study for their collaboration, the staff at the screening centre, the laboratory at the Department of microbiology and the laboratory at the Department of medical biochemistry, University Hospital of North Norway and the laboratory at Haukeland university hospital. We also thank Bjørg C Haldorsen for technical assistance and Åshild Bjørnerem for excellent advice on sex-steroids.
Author contributions
A.-S. F., C. S. N., G. S. S. and G. G. contributed with the conception and design of the work. B. H. performed biochemical analysis of sex-steroids and binding proteins. J. U. E. S. performed microbiological analysis of nasal samples. A.-S. F., D. B. S., K. O. and L. S. A. interpreted the data. D. B. S. performed the statistical analysis and wrote the first draft. All authors read and approved the final manuscript. The corresponding author attests that all listed authors meet authorship criteria.
Financial support
This work was supported by the Northern Norway Regional Health Authority (grant number HNF1457-19) and the Odd Berg Group Medical Research fund 2007. The funding sources had no part in the design of the study and collection, analysis and interpretation of data or in writing the manuscript.
Conflict of interest
None.
Ethical standards
Tromsø6 was approved by the Regional Committee for Medical and Health Research Ethics (REK) and the Norwegian Data Protection Authority. The present analysis including all methods was approved by the Regional Committee for Medical and Health Research Ethics (2018/1975/REK nord). The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Consent to participate
Participants in Tromsø6 were informed to read the information folder before the survey and signed the informed consent form when they attended the study sight. The study does not include data from participants with their declaration of consent withdrawn after participation.
Data availability statement
The data that support the findings of this study are available from The Tromsø Study but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon request and with permission of The Tromsø Study. Proposals for data should be directed to tromsous@uit.no. Statistical analysis and consent form will be available on request. Proposals should be directed to dina.b.stensen@uit.no.



 Open access
Open access