



The last stage of palliative surgeries for patients with a single effective ventricle, also known as "Fontan procedure," has survived to the present day with devoted and ongoing modifications since the 1970s to reduce both mortality and morbidity. The creation of a total cavopulmonary connection enabled many children with fatal defects to live into adulthood. Even though mortality has improved, non-physiological flow dynamics constituted the remaining problems related to morbidity. By the advances in surgical technique and patient follow-up since the first Fontan operation, the current interest is not to ensure the survival of patients, but to increase their quality of life after surgery. Among morbidities, prolonged pleural effusion following the Fontan operation is the most common complication that is responsible for increased length of hospital stay and increased time with draining tube thoracostomies. More importantly, prolonged pleural effusion, which manifests in the early post-operative period, may be a precursor of a failing Fontan circulation that may consequently cause the eruption of other "hard-to-cope-with" entities such as plastic bronchitis, protein-losing enteropathy, thromboembolism etc. Reference Menon, Chennapragada, Ugaki, Sholler, Ayer and Winlaw1–Reference Rogers, Glatz and Ravishankar3 For these reasons, determining appropriate candidacy for "ideal" Fontan operation and predicting patients who will experience a problematic post-operative course is crucial. In our institution since 2018, a medical treatment protocol, which resulted to be effective in terms of decreasing the total drainage, duration of pleural effusion, and length of hospital stay, applied to all patients immediately after Fontan operation. Reference Ergün, Yıldız and Ayyıldız4 The purpose of this study is to enlighten the factors (among numerous pre-operative, operative, and post-operative variables) affecting the effusion by reviewing the data of patients whose hospitalisation was complicated by prolonged pleural effusion despite the protocol.
Materials and method
Patient group and data
The medical data of 69 patients who underwent Fontan operation for the end-stage palliation of single ventricle physiology at Mehmet Akif Ersoy Training and Research Hospital between June 2018 and December 2020 and survived were reviewed. The study was approved by the review board of our institution. We analysed baseline characteristics, pre-operative clinical data, haemodynamic data from cardiac catheterisation, operative, and post-operative variables in all patients (146 variables). The study period was started from June 2018 which is the date we initiated a modified protocol of ours that was applied to all patients immediately after Fontan operation (Table 1). Prolonged pleural effusion was defined as the need for a chest tube for >7 days despite the protocol (prolonged pleural effusion group and non-prolonged pleural effusion group). We compared data between the two groups. All candidates were routinely evaluated with cardiac catheterisation in our institution prior to Fontan operation, and the following data were collected: pulmonary vascular resistance, systemic vascular resistance, mean pulmonary artery pressure, end-diastolic pressure of the systemic ventricle, and transpulmonary gradient. We also checked the distribution and calibration of the pulmonary arteries with Z-scores, pulmonary venous return; the systemic and hepatic venous return, bidirectional Glenn anastomosis, systemic outflow obstruction, aortopulmonary or veno-venous collaterals; and pulmonary arterio-venous fistulae. For the purpose of revealing risk factors associated with prolonged pleural effusion based on catheterisation data, patients were subdivided into “high-risk” and “low-risk” groups (high risk is defined by either of pulmonary vascular resistance/ systemic vascular resistance >0.3, mean pulmonary artery pressure >15 mmHg, end-diastolic pressure of the systemic ventricle >12 mmHg, transpulmonary gradient >10 mmHg, right pulmonary artery or left pulmonary artery Z-score <−2.00). Patients with elevated mean pulmonary artery pressure and/or pulmonary vascular resistance/systemic vascular resistance ratio as mentioned above are treated with a pulmonary vasodilator, typically sildenafil± bosentan, and are reassessed with cardiac catheterisation after 6–12 months of treatment.
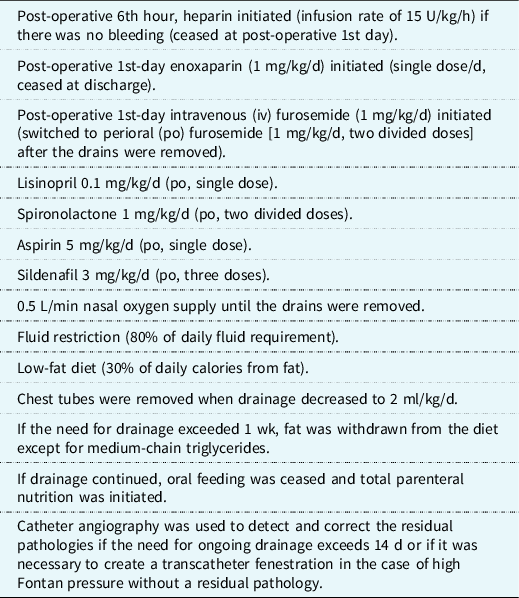
Table 1. Istanbul Mehmet Akif Ersoy Training and Research Hospital, Fontan protocol (modified Wisconsin protocol).
Surgical technique
The extracardiac Fontan operation was routinely performed for end-stage palliation in all patients, and an intra-extracardiac Fontan operation was performed in patients with isomerism and unusual systemic and pulmonary venous patterns. The procedures were performed under normothermic or mild hypothermic cardiopulmonary bypass. Cardioplegic arrest was used only in cases of concomitant intracardiac procedures. The pulmonary arteries were reconstructed as necessary. All remaining pulmonary antegrade flow was occluded at the Fontan operation, if not previously. Fenestration is performed in cases with moderate or severe atrioventricular valve regurgitation or high pulmonary vascular resistance, end-diastolic pressure of the systemic ventricle, and cases with comparably older age at Fontan operation. For eligible patients, a 4 mm fenestration was created in the conduit.
Post-operative follow-up
For ICU follow-up, our institutional routine is to extubate the patient as early as possible, apply low positive end expiratory pressure, if the patient remains intubated, and maintain a positive fluid balance for the first 24 hours to assure a fully loaded Fontan system which is a passive conduit. At immediate post-operative period, we applied the aforementioned protocol. Reference Cava, Bevandic, Steltzer and Tweddell5,Reference Pike, Okuhara, Toyama, Gross, Wells and Starnes6 Chest tubes were removed if the drainage converts into serous character, chest X-ray demonstrating no significant pleural collection, and drainage was <2 ml/kg/day. A delicate diet was applied to patients if the pleural drainage prolonged and exhibited chylous character, fat was withdrawn from the diet except for medium-chain triglycerides, and total parenteral nutrition was initiated if chest tubes were not withdrawn in the post-operative 14 days. Catheter angiography was performed if the drainage period exceeded 14 days and total parenteral nutrition brought no help. Octreotide use was preserved for cases with substantial and prolonged chylous output. We continued the low-fat diet for 6 weeks after removal of the last chest tube.
Statistical analysis
Data analyses were performed using SPSS 25 software and were presented as median values (and range). The χ2 test was used for categorical variables, and the unpaired Student’s t-test was used for continuous variables that were distributed normally. Non-parametric continuous variables were analysed using the Wilcoxon rank-sum test/Mann–Whitney U-test. Univariate analysis was performed for possible variables to predict prolonged pleural effusion. Those variables with a p value <0.05 were considered to be statistically significant.
Results
Pre-operative variables
Baseline characteristics of the patients are displayed in Table 2. In detail, 40 patients were female (58%), the median age at Fontan operation was 4.9 years (range 2.5–26), and the most frequent main diagnosis was tricuspid atresia (n:13, 19%). Ten patients among prolonged pleural effusion group (35%) had pulmonary atresia coexistent with the main diagnosis. Dominant ventricle was left in 39 (56%), and total anomalous pulmonary venous drainage was observed in 4, mostly supracardiac and concomitantly in patients with right atrial isomerism and right ventricular dominance (6%). Among those 4 patients with total anomalous pulmonary venous drainage, only one patient had prolonged pleural effusion. Only 1 of 6 patients with left atrial isomerism (17%) had prolonged pleural effusion and prolonged for more than 14 days. Atrioventricular valve regurgitation figures before Fontan operation were as follows: the most common was mild regurgitation in 28 of all patients (40%) and in 11 of patients (39%) suffering from prolonged pleural effusion. No statistically significant difference was found between two groups in terms of atrioventricular valve regurgitation. The median age at Glenn shunt operation was 18.9 months (2-76), and age at Glenn shunt surgery was not found to be a risk factor for having prolonged pleural effusion when patients were further divided into 3 subgroups according to their age at Glenn shunt operation (4–6 m, 6–12 m, 12 m<)(p:0.57).
Table 2. Pre-operative demographic data.
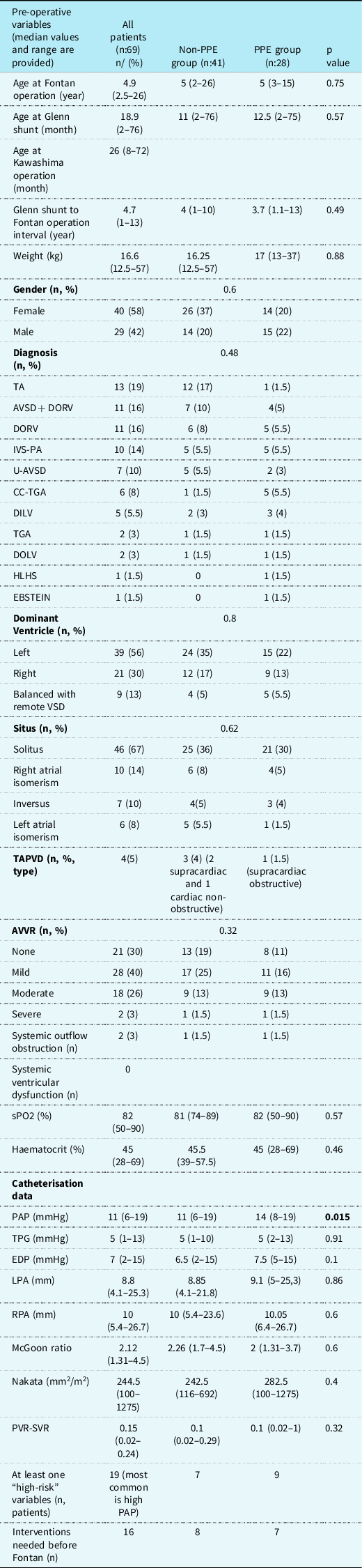
Abbreviations: TA, tricuspid atresia; u-AVSD, unbalanced atrioventricular septal defect; DORV, double outlet right ventricle; IVS-PA, intact ventricular septum-pulmonary atresia; cc-TGA, corrected transposition of great arteries; DILV, double inlet left ventricle; TGA, transposition of great arteries; DOLV, double outlet left ventricle; HLHS, hypoplastic left heart syndrome; VSD, ventricular septal defect; TAPVD, total abnormal pulmonary venous return; AVVR, atrioventricular valve regurgitation; PAP, mean pulmonary artery pressure; TPG, transpulmonic gradient; EDP, systemic ventricular end-diastolic pressure; LPA-RPA, left and right pulmonary arteries; PVR-SVR, pulmonary and systemic vascular resistance.
The median time interval from Glenn shunt to Fontan operation was 4.7 years (1–13 years) in the entire cohort and was not significantly different between prolonged pleural effusion and non-prolonged pleural effusion groups. Fontan operation was performed in six patients (8.7%) over the age of 10, and 4 of these patients (67%) had prolonged pleural effusion, whereas in two patients prolonged pleural effusion lasted longer than 14 days. Two patients had systemic ventricular outflow tract obstruction, none of whom had prolonged pleural effusion after Fontan operation. Systemic ventricular functions were preserved in all patients pre-operatively. Median saturation and haematocrit values were 82 and 45%, respectively. Laboratory indices were within the normal range in two groups before Fontan operation and deviations from initial pre-operative values are covered in post-operative data part comparably. As for catheterisation data, the median mean pulmonary artery pressure was 11 mmHg (6–19) and the median transpulmonary gradient was 5 mmHg (1–13). Pre-operative mean pulmonary artery pressure was elevated in prolonged pleural effusion group (p:0.015). Other catheter derived data were shown in Table 2. The most common angiographically obtained “high-risk” factor was elevated mean pulmonary artery pressure (four patients-13%) in prolonged pleural effusion group, and in two patients, both of whom had more than one risk factor, pleural effusion lasted longer than 14 days. Among all, 21 patients (30%) had prolonged pleural effusion despite having no risk factor at all. Seven patients out of 11 (70%) with effusion lasted more than 14 days had no risk factor. Anti-pulmonary hypertension treatment was initiated in six patients (three of whom had prolonged pleural effusion ) as the mean pulmonary artery pressure was more than 15 mmHg in the pre-Fontan catheter. Ten patients (15%), none of whom had prolonged pleural effusion, required 16 interventions at diagnostic angiography before Fontan operation (five veno-venous collateral occlusions and four major aortopulmonary collateral artery occlusions being the most common). Pre-operative stage 1 preferences and concomitant procedures are listed in Table 3, and palliation preferences were not statistically associated with prolonged pleural effusion. Nevertheless, no connection could be established in terms of prolonged pleural effusion, presence of collaterals requiring transcatheter intervention, and pulmonary artery Z-scores at pre-operative catheterisation between the group whose antegrade pulmonary flow was occluded at the Glenn shunt stage and the group that was not (p:0.34 for prolonged pleural effusion, p: 0.7 for fistula occlusion, p: 0.5 for z-scores).
Table 3. Initial palliation references at Stage 1 and Stage 2 (Glenn shunt) data.

Abbreviations: RVOT, right ventricular outflow tract; AVV, atrioventricular valve; TAPVD, total abnormal pulmonary venous return.
Operative and peri-operative data
Extracardiac Fontan operation was applied to all except seven patients who underwent intra-extracardiac Fontan. Fenestration was performed in six (8%) patients during the procedure, three of whom had prolonged pleural effusion post-operatively. There was no statistically significant difference between the groups in terms of cardiopulmonary bypass, fenestration rate, and aortic cross-clamp time. Thirty-six (52%) patients underwent an additional concomitant procedure during the Fontan surgery. Atrioventricular valve repair was the leading procedure (n = 9, 13%), which was followed by pulmonary artery reconstruction (n = 6, 8%), whereas 33 patients (48%) did not need any additional manipulation (Table 4). Among 69 patients, 28 (40%) had prolonged pleural effusion, whereas 11 (16%) had effusion that lasted longer than 14 days. Post-operative extubation was at median of 6 hours (1–26). The median post-operative ICU stay and hospital stay were 3 days and 10 days, respectively. Other post-operative variables comparable to both groups are provided in Table 4. [Among numerous variables, statistical significance between the prolonged pleural effusion and non-prolonged pleural effusion groups was achieved in pre-operative mean pulmonary artery pressure; post-operative albumin, C-reactive protein and gamma-glutamyl transferase levels, and amount of effusion per day].
Table 4. Operative and post-operative data.

Abbreviations: SCV, superior caval vein; ICV, inferior caval vein, RA, right atrium; CPB, cardiopulmonary bypass; ACC, aortic cross-clamp; VSD, ventricular septal defect; ASD, atrial septal defect, CRP, C-reactive protein; GGT, gamma-glutamyl transferase.
*: “early” represents the post-operative day 0 to 3, “late” represents follow-up interval in the patient ward. Only statistically significant laboratory indices were provided.
Catheter angiography was performed in all patients with an extraordinary post-operative clinical course such as failure of extubation, prolonged effusions, unexplained hypotension, desaturation, or decreased contractility of single ventricle. Six patients required catheter angiography within the post-operative 30 days [two diagnostic purposes, three transcatheter fenestration (one due to spontaneous closure of surgical fenestration) and one fenestration closure due to ischaemic cerebrovascular event].
Readmissions within post-operative 30 days were due to recurrent pleural effusion for 8 patients (all were managed medically), surgical site infections treated with intravenous antibiotics for 2, supraventricular arrhythmia that needed cardioversion for 1, ascites that was later complicated by protein-losing enteropathy for 1. One patient, who had bilateral bidirectional Glenn shunt operation at 6 years old, underwent Fontan operation a year afterwards with the diagnoses of right atrial isomerism, unbalanced common atrioventricular canal defect with severe atrioventricular valve regurgitation. Her post-operative period was complicated with intractable bilateral pleural effusion that required initial thoracic duct ligation which resulted inconclusively and sclerosing agent administration therapy to lymph nodes afterwards.
Discussion
Despite the mortality following Fontan operation has being reduced, morbidity remains considerable. Real cause of persistent effusions is obscure and likely multifactorial. We apply a medical treatment protocol that was reported to reduce amount of total pleural drainage in the immediate post-operative period after Fontan procedure since 2018. Reference Ergün, Yıldız and Ayyıldız4 Nevertheless, still some patients have prolonged pleural effusion, which was the source of inspiration for the current study to uncover the risk factors for prolonged pleural effusion despite protocol. We defined effusion "prolonged" >7 days contrast to many published series that defined it as >14 days. Reference Tran, Le and Vo7,Reference Rito, Al-Radi and Saedi8 Although this explains slightly elevated rate of our cohort group for prolonged effusion (%40), which is still consistent with the literature, we claim that “7 days” was a more appropriate cut-off interval for defining “prolonged” to detect and intervene problems in the Fontan circulation earlier and to reduce length of hospitalisation and susceptibility to infections. Reference Rito, Al-Radi and Saedi8–Reference Kim, Ko and Byun10
Appropriate timing for Fontan completion is associated with post-operative outcomes and prolonged effusions. Iyengar et al. from Anzac registry including 1071 Fontan patients claim that early Fontan operation does not bring superiority and later age at surgery seems to be associated with worse late functional outcomes but also worse early outcomes. Reference Iyengar, Winlaw and Galati2 Our cohort also showed that the incidence of prolonged pleural effusion increased in patients who had Fontan operation at older age, though it did not reach a statistical significance due to limited number of patients. Surgical timing is also important at Glenn shunt stage. Although age at Glenn shunt did not differ in terms of prolonged pleural effusion, we suggest that Glenn anastomosis plays a crucial role by partially unloading the systemic ventricle and should not be performed too late once pulmonary arterial development is considered sufficient. Reference Ganigara, Prabhu, Varghese, Pavithran, Valliatu and Kumar11
As for morphology, the frequency of prolonged pleural effusion has been reported to be higher in right ventricular dominant circulations or specifically in patients with hypoplastic left heart syndrome in the literature. Reference Iyengar, Winlaw and Galati2,Reference Gupta, Daggett, Behera, Ferraro, Wells and Starnes9,Reference Gaynor, Bridges and Cohen12,Reference Julsrud, Weigel and Van Son13 Even though we had only one patient with a primary diagnosis of hypoplastic left heart syndrome, tricuspid atresia is less likely to be a risk factor for prolonged pleural effusion compared to other pathologies in the current study. From this point of view, it can be speculated that a ventricle with preserved systemic ventricular functions and congenitally programmed to support systemic circulation is a more suitable candidate for Fontan physiology. Another anatomical consideration is the competence of pulmonary vasculature to adopt total cavopulmonary anastomosis. Lo et al. claimed that pulmonary atresia was a predictor of prolonged pleural effusion which we approve by having 35% of pulmonary atresia in our patient group suffering from prolonged effusion. Reference Rito, Al-Radi and Saedi8 The underlying pathology may be the incomplete adaptation process in the postnatal period of the vascular bed that was not sufficiently perfused in the intrauterine period even though pulmonary vascular resistance calculations and pulmonary artery Z-scores were proven to be within normal range.
Atrioventricular valvular regurgitation is another concern in patients undergoing Fontan operation, with most patients having mild degree of regurgitation before surgery in both literature and in our cohort. Reference Tran, Le and Vo7,Reference Podzolkov, Chiaureli and Yurlov14 Moderate to severe regurgitation status is considered for concomitant atrioventricular valve repair at surgery in our institution to preserve diastolic functions of the "long-time sufferer" ventricle though concomitant atrioventricular valve repair and pre-operative moderate/severe atrioventricular valve regurgitation were not related to prolonged pleural effusion in the present study. Tran et al. published atrioventricular valve regurgitation as a pre-operative variable for prolonged pleural effusion, and Podzolkov et al. suggested correction of moderate to severe regurgitation not after Fontan completion despite the contradictory findings on the appropriate timing of atrioventricular valve repair in univentricular hearts. Reference Tran, Le and Vo7,Reference Podzolkov, Chiaureli and Yurlov14
New "Fontan circulation" is an altered form of haemodynamics and strictly intolerant to stenosis at any site through the vascular tubing system including pulmonary arteries, systemic ventricular outflow tract, any of which needs to be corrected before or at Fontan stage. For this reason, we prefer to perform cardiac catheterisation before Fontan operation for evaluation of aforementioned concepts. We also welcome new imaging techniques in this patient population to allow us to identify pre-operative high-grade abnormal thoracic lymphatic perfusion as a risk factor for developing early post-Fontan complications. Currently, we initiated to obtain cardiac MRI of these patients pre-Fontan routinely. Among variables extracted from catheterisation data, pre-operative mean pulmonary artery pressure, which was also the most common angiographically obtained "high-risk" factor in patients with prolonged pleural effusion, was found to be elevated in prolonged pleural effusion group and intraoperative measurements were found mostly within normal limits even in patients with prolonged pleural effusion and elevated mean pulmonary artery pressure at pre-Fontan catheterisation maybe due to effect of general anaesthesia on pulmonary vascular resistance. Lo rito et al. with 324 patients claimed that a 5 mmHg increment in pre-Fontan mean pulmonary artery pressure was associated with a 25% increase in the duration of chest tube requirement. Reference Rito, Al-Radi and Saedi8 Sasaki et al. reported that increased mean pulmonary artery pressure was associated with prolonged length of stay among their 218 patients. Reference Sasaki, Dykes and Sosa15 Therefore, though there was no absolute cut-point, a pre-operative mean pulmonary artery pressure ≥15 mmHg is a reliable data for early outcomes and prolonged pleural effusion as many publications support. Reference Rogers, Glatz and Ravishankar3,Reference Rito, Al-Radi and Saedi8 Another important finding of ours that patients with more than one catheterisation "high-risk" factor had effusion lasted more than 14 days. Interestingly, among all, 30% had prolonged effusion despite having no angiographic risk factor at all. Seven patients out of 11 (70%) with effusion lasted more than 14 days had no risk factors. To summarise, the absence of a risk factor does not exclude the possibility of early complications, whereas high mean pulmonary artery pressure in the pre-Fontan catheter can be considered as predictive of prolonged pleural effusion.
Currently, extracardiac conduit use is becoming the preference of anastomosis in patients undergoing Fontan surgery. However, which patient should be fenestrated is still in need for consensus. Fenestration rates were similar between two groups in our study. In many previous reports, fenestration has been associated with better outcomes, including a decreased risk of death, prolonged pleural effusion, and longer hospitalisation. Lemler et al. performed the prospective randomised trial to evaluate the clinical utility of fenestration in patients with standard pre-operative risk profiles for 49 consecutive Fontan operations. They concluded that baffle fenestration improves short-term outcome in standard-risk patients by decreasing pleural drainage, length of hospital stay, and need for additional post-operative procedures. Reference Lemler, Scott, Leonard, Stromberg and Ramaciotti17 In our unit, we suggest that opening fenestration in risky patients would be appropriate bearing the decrease in saturation and the risk of embolic phenomena in mind.
The relationship between the course of laboratory parameters and prolonged pleural effusion in the post-operative period raised curiosity, since there are not many publications on this subject. At the same time, the opening of the pleural cavities during the operation, the subsequent inflammatory process, and the increase in vascular permeability as a result of possible pressure changes in the lymphatic system contribute to the formation and prolongation of pleural effusion. Harmoniously, it was demonstrated that in post-operative Fontan patients, the inflammation within the pleural space, which is significantly greater when compared to controls undergoing cardiopulmonary bypass, is out of proportion to the systemic inflammation. Reference Goldstein, Beshish and Bush18 Our findings indicate that post-operative albumin levels (late) were lower, whereas both early and late C-reactive protein levels were elevated in prolonged pleural effusion group. Although high C-reactive protein levels in the late period indicates ongoing inflammation and low albumin levels indicates protein wasting due to capillary leakage secondary to inflammation, considering the contribution of variables such as infection, fluid balance, blood transfusions, diuretic therapy in the post-operative period, it is debatable how much these findings can be adapted to daily practice. However, early C-reactive protein levels, post-operative 0–3 days, may be a good predictor. In this context, we postulate that inflammation and vascular permeability within the pleura and factors affecting this permeability such as cardiopulmonary bypass and infections are effective in prolonging the effusion. Moreover, providing an infection-free post-operative follow-up and to strengthen the medical treatment with corticosteroids and anti-inflammatory agents in cases without active infection are becoming prevalent in our unit. In spite of application to a small number of cases yet, the decrease in duration of effusion and hospital stay appears encouraging.
Through this study, we tried to predict prolonged effusion after Fontan surgery over conventional variables due to the retrospective design. Nevertheless, we are well aware of that in order to approach perfection in Fontan physiology innovative variables need to be involved. Methods such as computational fluid dynamics initiating the evaluation from Glenn shunt stage even possibly from the palliation period to reveal the haemodynamics in the pulmonary arteries, MRI before Fontan to evaluate lymphatic system which is of great importance and maybe utilisation of “flow study” to evaluate the pulmonary arterial vasculature readiness by simulating a Qp/Qs of 1 in the intraoperative period would be our future interests.
Conclusion
Pleural effusion after the Fontan procedure continues to be a challenging problem. Therefore, risk-stratifying patients for Fontan candidacy and implementing consistent post-operative care with a standardised protocol targeting the unique physiology of Fontan patients are crucial. Elevated pre-operative mean pulmonary artery pressure; post-operative elevated C-reactive protein; and low albumin levels were related with prolonged pleural effusion in the current study.
Limitations
This study was limited by its retrospective and single-centre design. Due to limited number of patients, multivariate model could not be constructed despite many variables being available. Although we had patients with infections or complicated with acute kidney injury during long stays in the ward, their statistical significance could not be considered due to the limited number of patients complicated with those entities.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of interest
None.
Ethics approval
Ethical approval was waived by the local Ethics Committee of University of Health Sciences in view of the retrospective nature of the study, and all the procedures being performed were part of the routine care.




