


Increased post-traumatic stress disorder (PTSD) rates have been well documented in children and adolescents exposed to warReference Thabet and Vostanis1 as well as children who experienced multiple childhood adversities such as family violence, various forms of child abuse and neglect and polyvictimisation.Reference Cloitre, Stolbach, Herman, Kolk, Pynoos and Wang2–Reference Copeland, Keeler, Angold and Costello4 More recently the interplay of war trauma and childhood adversity has been examined on a national scale,Reference Karam, Mneimneh, Karam, Fayyad, Nasser and Chatterji5 finding that childhood adversities were strongly related to war events.Reference Itani, Haddad, Fayyad, Karam and Karam6 Furthermore studies assessing the role of war exposure or childhood adversities reported either an independent contribution of each to PTSD symptoms,Reference Schiff, Pat-Horenczyk, Benbenishty, Brom, Baum and Astor7, Reference Dubow, Huesmann, Boxer, Landau, Dvir and Shikaki8 or reported an additive effect when war events and childhood adversities were experienced together.Reference Catani, Schauer and Neuner9, Reference Okello, De Schryver, Musisi, Broekaert and Derluyn10 However, the relative contributions of war trauma and childhood adversities regarding the development of PTSD is still far from settled as some studies reported greater weight of childhood adversities compared with war exposure in predicting PTSD,Reference Catani, Schauer and Neuner9 whereas others showed a more complex relationship where the magnitude of childhood adversities was the main driver of PTSD symptoms, with war predicting PTSD levels only when childhood adversity was low.Reference Okello, De Schryver, Musisi, Broekaert and Derluyn10
Current understanding about the influence of environmental sensitivities in the response to trauma
Importantly, individual characteristics can also influence children's response to adversities and trauma. Several models of person–environment interaction and associated empirical studies show that more sensitive individuals are more vulnerable to the negative effects of adversity (i.e. diathesis–stress, ZuckermanReference Zuckerman11, Reference Monroe and Simons12) but also more likely to benefit from supportive ones (i.e. vantage sensitivity and differential susceptibilityReference Belsky and Pluess13). Such sensitivity to environmental influences can be measured reliably with a validated questionnaireReference Pluess, Assary, Lionetti, Lester, Krapohl and Aron14 that has been shown to predict the response to school-based psychological programmesReference Pluess and Boniwell15, Reference Nocentini, Menesini and Pluess16 and parenting qualityReference Slagt, Dubas, van Aken, Ellis and Dekovic17 (i.e. more sensitive children show a stronger response to both negative and positive environmental exposures). However, the role of environmental sensitivity in the response to war experience has not yet been examined.
The war in Syria has been raging since 2011, and this has resulted in more than 1.5 million Syrians taking refuge in Lebanon. Consistent with an ecological framework, multiple factors are at play in producing the final clinical picture of PTSD.Reference Betancourt and Khan18, Reference Bronfenbrenner19 Therefore, it is important for researchers and clinicians alike to have a comprehensive look at the various factors that affect PTSD. This study tries to fill a gap in this field by examining the effects of war trauma, coexisting childhood adversities and the individual trait of sensitivity as well as their interplay in predicting PTSD in Syrian children and adolescents based in Lebanon.
Method
Participants
The participants were Syrian refugee children participating in a mental health assessment in Lebanon with an intervention component delivered by teachers to Syrian and Lebanese students in their classroom. The intervention aimed at building resilience among Syrian refugee children and adolescents enrolled in Lebanese public schools in regions recommended by the Ministry of Social Affairs and the Ministry of Higher Education as having low psychosocial support from non-governmental organisations because of the Syrian influx (personal communication with Ministry of Social Affairs personnel). After obtaining written parental consent and student assent, data were collected from a total of 549 Syrian children and adolescents attending schools in the following regions: Sidon, Metn suburbs of Beirut, city and caza of Aley, the district of Chiyah in the Beirut South suburbs and the city of Jounieh and its suburbs.
All public schools in these regions were listed and only schools containing grades 4–7 (ages 7–17 years) and with a student population size greater than 100 were enrolled in the study. Following the recruitment visits to the schools’ principals, 32 schools out of 54 agreed to participate in the study. The reasons for refusal were: the unavailability of teachers to participate in the intervention or the existence of other psychosocial programmes that the school had already committed to. One school was excluded later as a result of problems in adherence with the research protocol. Internal review board approval was obtained from the Internal Review Board of the Balamand University Faculty of Medicine.
Measures
A total of 48 school teachers and 12 field workers were trained by professionals from the Institute for Development, Research, Advocacy and Applied Care (Beirut, Lebanon) on the contents of the self-filled questionnaires to be completed by the students. Details on the purpose and the aim behind collecting information on students’ sociodemographic details, traumatic event exposure (war and childhood adversities), sensitivity as well as PTSD symptoms were explained. Moreover, the questionnaires were discussed thoroughly and the importance of following instructions while filling in the questionnaires was highlighted. The data-collection phase took place over two classroom sessions. In order to ensure the quality of the data collected was accurate and thorough, we assigned field workers to individual classrooms to assist the teachers during the data collection. Any problems encountered on site were directly reported by the field workers to the project manager.
PTSD symptoms were assessed using the PTSD Reaction Index (PTSD-RI) for DSM-IV, which includes a total of 20 post-traumatic stress symptom items rated on a scale of 0–4.Reference Pynoos, Rodriguez, Steinberg, Stuber and Frederick20 Scores were classified as ‘mild PTSD reaction’ (total score 12–24), ‘moderate’ (25–39), ‘severe’ (40–59), and ‘very severe’ (above 60). The PTSD-RI total score has also been used extensively in various Arab populations including children and adolescents in Gaza and Kuwait.Reference Thabet, Abed and Vostanis21–Reference Nader, Pynoos, Fairbanks, Al-Ajeel and Al-Asfour23
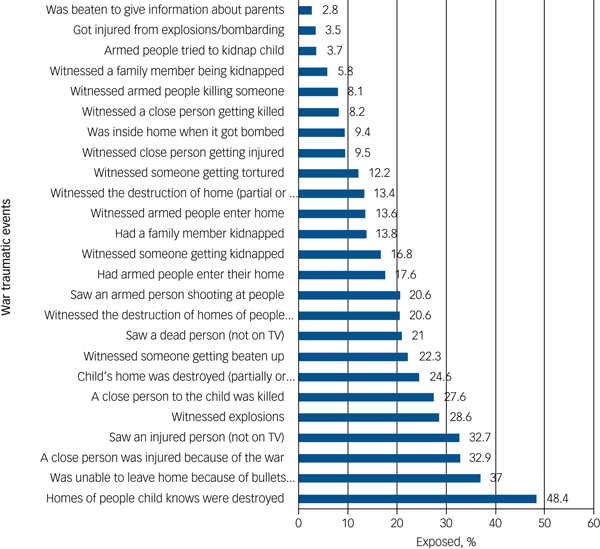
War exposure was measured with a checklist of 25 items with a corresponding score of 1 for every war item children have experienced. The list of war exposure items was created by our group following focus group discussions with Syrian refugee mothers based on their experiences and reports of the most common events encountered by Syrian children and their families. War items ranged from being unable to leave home because of bullets and bombings to witnessing people getting tortured and/or dying (Fig. 1).
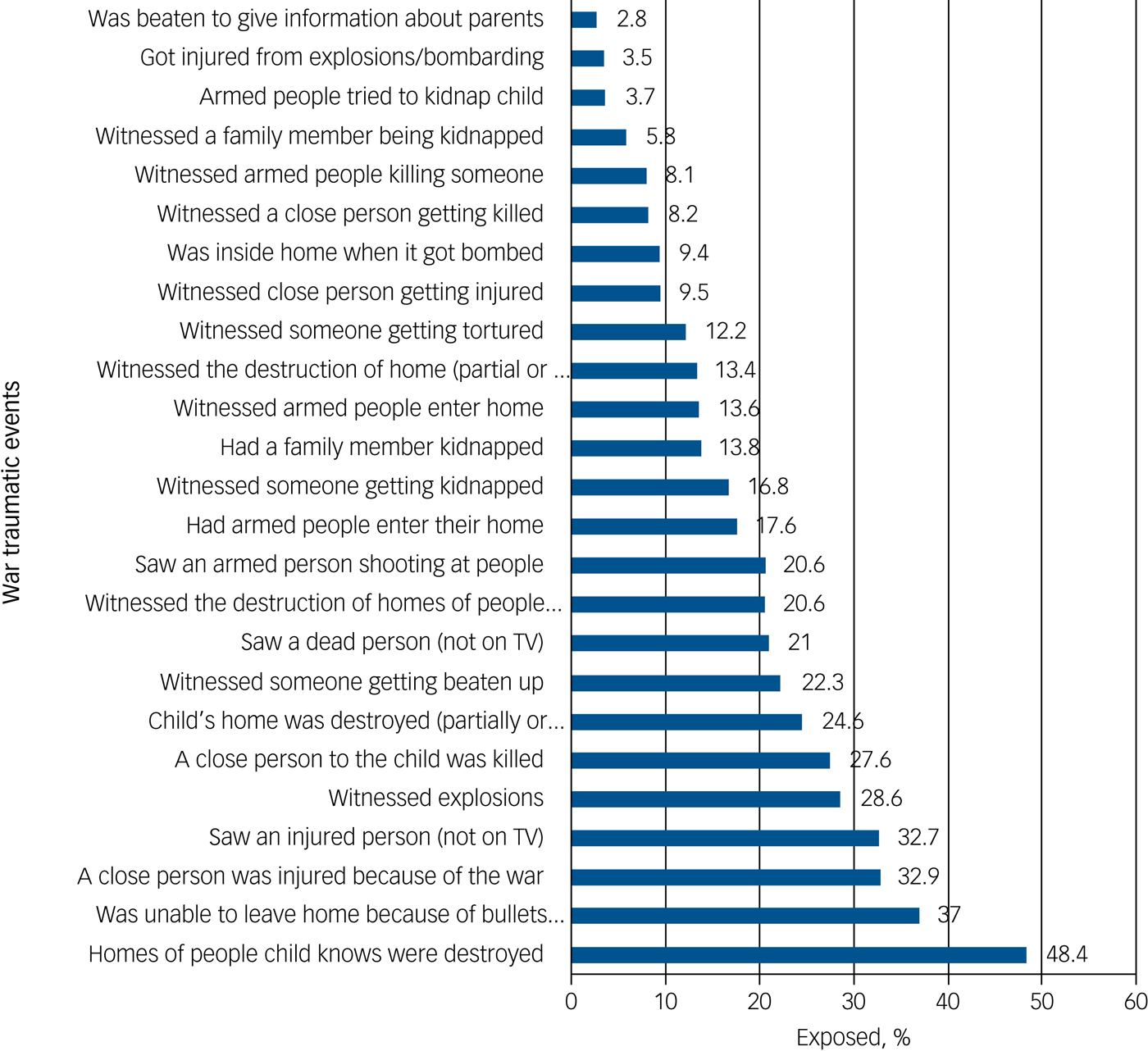
Fig. 1 Exposure to traumatic war events (n = 549).
The instrument for childhood adversities included a total of 29 items rated as 0 (never/rarely), 1 (sometimes) or 2 (often/always) (total possible score range: 0–58) (Fig. 2). The childhood adversities measure was composed of items from the ISPCAN Child Abuse Screening Tools (ICAST) (17 items),Reference Runyan, Dunne, Zolotor, Madrid, Jain and Gerbaka24 as well as a list of adversities (10 items) previously created by our group based on focus groups discussions with mothers, and two additional items related to childhood neglect based on the Composite International Diagnostic Interview.Reference Kessler and Ustun25 ICAST adversities were collected with the following responses: never (score of 0), sometimes in the past year (score of 1), always in the past year (score of 2), and ‘not in the past year, but happened in the past’. These responses were re-coded in the childhood adversities index as never (0), sometimes (1) or always (2). For respondents who chose the option ‘not in the past year but happened in the past’ for any item, a score (between 0 and 2) was imputed for them based on their responses to other ICAST items that happened during the past year.
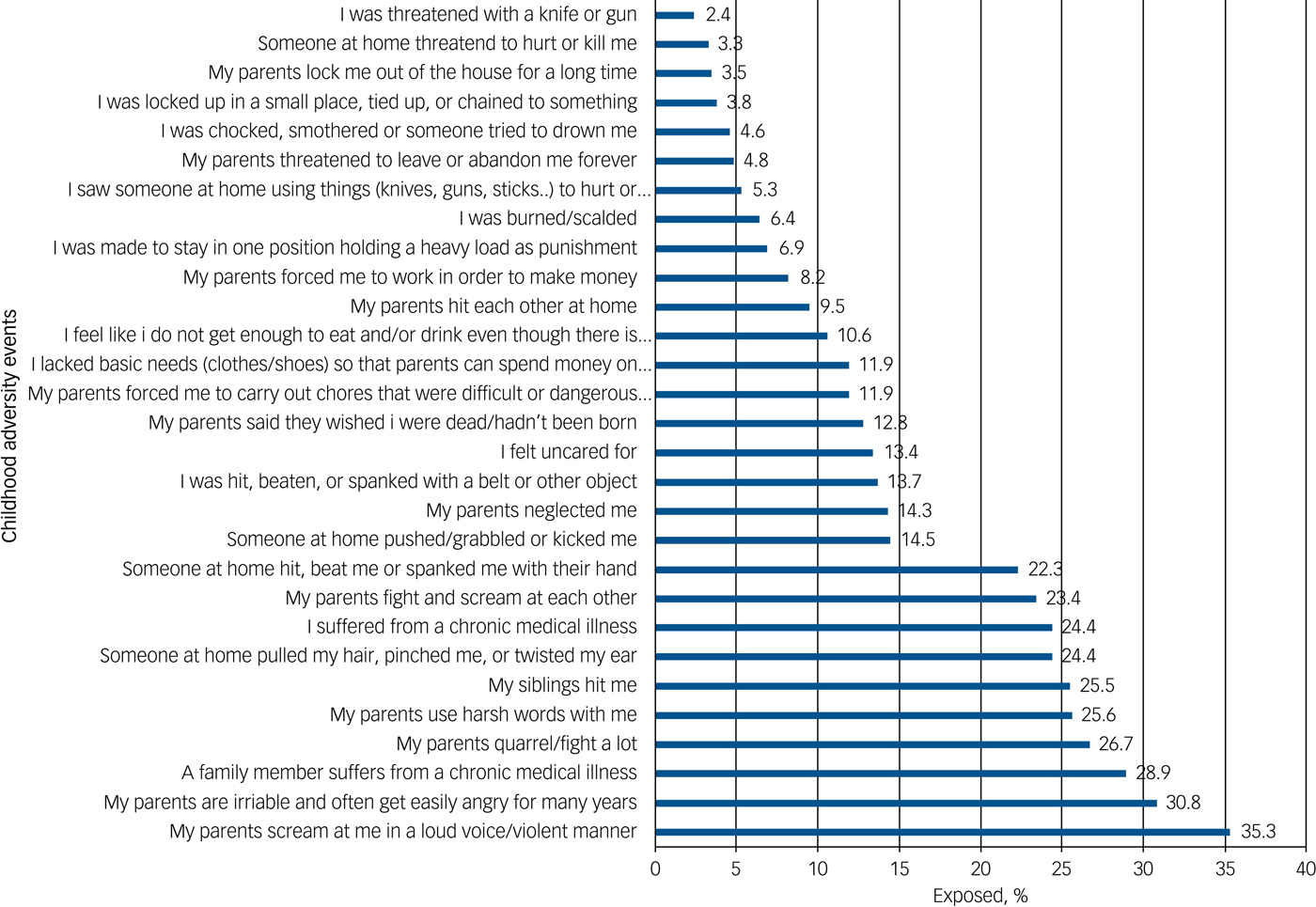
Fig. 2 Exposure to childhood adversity events (n = 549).
Sensitivity was measured using the Highly Sensitive Child Questionnaire (HSC)Reference Pluess, Assary, Lionetti, Lester, Krapohl and Aron14 which includes a total of 12 items each rated on a scale of 0 to 6 (0, do not agree; 3, agree moderately; 6, totally agree) (total range score: 0–72) and reflects three factors: (a) the ease of excitation factor that reflects being easily overwhelmed, (b) low sensory threshold that captures unpleasant sensory arousal and (c) aesthetic sensitivity that measures sensitivity to aesthetic aspects of the environment. For the current analysis we used the total score as recommended by the authors of the scale.Reference Pluess, Assary, Lionetti, Lester, Krapohl and Aron14 The HSC scale was translated by our group into Arabic and back-translated into English followed by focus group discussions and reviewed by an expert panel (E.G.K., J.A.F., C.C.T., A.N.K., Y.C.H) to resolve any disagreements. The questionnaire was then delivered to a community group of Lebanese and Syrian children and adolescents to get their feedback about the wording and the meaning of the questions. The final form was agreed upon by the expert panel. Test–retest reliability was run on a sample of 27 Syrian refugee children aged between 8 and 13 years who were attending social developmental centres with their mothers. Time between test 1 and test 2 was 2 weeks. Test–retest reliability of the Arabic HSC was good, with an intraclass correlation coefficient of 0.73 (P<0.001). Based on the distribution of sensitivity, three levels were created by dividing its distribution into tertiles: low, middle and high sensitivity.
Statistics
We used descriptive statistics to determine the sample's characteristics, the rate of exposure to war and childhood adversities, and the severity levels of post-traumatic stress symptoms among the total sample of Syrian children and adolescents. An ANOVA test was conducted to analyse the differences in mean scores of war exposure among varying childhood adversity levels, and to further verify their co-occurrence (war exposure and childhood adversities) a bivariate linear regression was conducted.
Moreover, a series of linear regression models were estimated using the PTSD-RI total score as the outcome (since numbers were too small to use the severity categories for PTSD). Initially, predictors of increasing PTSD scores were established by calculating bivariate linear regression models. To assess the contribution of war exposure and childhood adversities to PTSD scores (as reported by the standardised β in the text), we conducted a series of additive linear regressions controlling for age and gender, followed by adding sensitivity to the model as a pre-final step. The final steps in these regressions examined the potential interactions between war exposure, childhood adversities and sensitivity. We report both unstandardised (b) and standardised (β). Bivariate and multivariate analyses were conducted using SPSS version 20, and significance was determined using a 95% confidence interval.
Results
Participant characteristics: sociodemographics, sensitivity and PTSD scores
The Syrian refugee children and adolescents (n = 549) were students from 112 classrooms also attended by Lebanese students: 39.5% were from grade 4, 27.0% from grade 5, 19.9% from grade 6 and 13.6% from grade 7. Their mean age was 11.9 years (s.d. = 1.6), with 54.8% being female.
Information on the length of time they had been in Lebanon was available for 259 Syrian children. This subsample was selected on the condition of having classrooms with five Syrian students or more and used in another comparative study with Lebanese students. About two-third had been in Lebanon for 5 years or less (161 children) at the time of the study and thus were more recent refugees and 81 had been in Lebanon for more than 5 years.
The mean PTSD-RI score was 14.1 (s.d. = 11.6, range 0–58). A total of 50.7% of children reported no reactions; 31.5% mild, 14.3% moderate and 3.5% severe post-traumatic stress reactions. There were no very severe reactions in this sample. There were 173, 179 and 175 respondents, respectively with low, middle and high sensitivity levels. Sensitivity scores in this sample were normally distributed with a mean score of 43.7 (s.d. = 11.9, range 7–72).
Exposure to war traumatic events
The mean number of war events experienced by Syrian refugee children was 4.53 (s.d. = 5.2, range 0–25). A total of 69.4% of the participants experienced at least one type of war event, with 25.7% reporting 1–3 war events and 43.7% reporting ≥4 war events. The war traumas experienced by the Syrian children and adolescents are listed in Fig. 1.
Exposure to childhood adversities
The mean score on the childhood adversity index was 3.99 (s.d. = 5.9, range 0–48) with 31.3%, 32.8% and 35.7% having a score of 0, 1–3 and ≥4 childhood adversities, respectively. A total of 68.6% of the sample reported at least one childhood adversity. The childhood adversities experienced by the Syrian children and adolescents are listed in Fig. 2.
Co-occurrence of war and childhood adversities
The mean number of war events increases significantly with increasing exposure to childhood adversities (P<0.0001). The mean number of war events increased from 2.74 (s.d. = 3.75) with 0 childhood adversities to 4.24 (s.d. = 4.52) with 1–3 childhood adversities and to 5.96 (s.d. = 5.86) with ≥4 childhood adversities. Moreover, a significant relationship exists between the number of war events and the number of childhood adversities (r = 0.266, P<0.0001).
Bivariate associations of age, gender, childhood adversities, war exposure and sensitivity with PTSD
At the bivariate level PTSD scores were significantly associated with age (β = 0.826, 95% CI 0.22–1.43, P = 0.007), childhood adversities (β = 1.019, 95% CI 0.88–1.16, P<0.0001), war exposure (β = 0.667, 95% CI 0.47–0.86, P<0.0001) and sensitivity (β = 0.166, 95% CI 0.08–0.25, P<0.0001). Gender was not significantly associated with PTSD (β = 0.365, 95% CI −1.62 to 2.34, P = 0.718).
Multivariate regressions
The additive multivariate regression model revealed independent main effects of both war exposure and childhood adversities in the prediction of PTSD. The effect of childhood adversities (standardised β = 0.490, P<0.0001) on PTSD scores was stronger than that of war (standardised β = 0.160, P<0.0001), at the bivariate level.
Introducing sensitivity into the multivariate model as shown in Table 1, also had a significant independent effect on PTSD (standardised β = 0.082, P = 0.039) (Table 1).
Table 1 Main and interaction effects on PTSD: Multivariate associations of age, gender, childhood adversities, war exposure and sensitivity predicting PTSD scores (n = 457)
We then investigated the interplay between war exposure, childhood adversities and sensitivity in the prediction of PTSD scores by evaluating the significance of interactions. The two-way interactions childhood adversities × war, war × sensitivity were significant in contrast to the non-significant interaction between childhood adversities and sensitivity. However, the three-way interaction between war, childhood adversities and sensitivity was significant (Table 1).
In order to interpret these findings, we stratified the participants by levels of childhood adversities and sensitivity to assess the effect of war exposure on PTSD scores across the nine categories representing the various levels of sensitivity and childhood adversities. We conducted a bivariate regression of war on PTSD.
At low childhood adversity exposure the effect of war on PTSD scores were: 0.016 (P = 0.933) at low sensitivity, 0.299 (P = 0.018) at middle sensitivity and 0.582 (P<0.0001) at high sensitivity. Among the middle childhood adversity exposure group, the effect of war on PTSD scores were: 0.125 (P = 0.439), 0.321 (P = 0.003) and 0.501 (P<0.0001) for low, middle and high sensitivity, respectively. At high levels of childhood adversities, the effect of war on PTSD scores were: 0.355 (P = 0.014) at low sensitivity, 0.374 (P<0.0001) at middle sensitivity and 0.321 (P = 0.019) at high sensitivity.
Results suggest that at low and middle levels of childhood adversity, the effect of war exposure on PTSD becomes stronger with increasing sensitivity. In contrast, at high levels of childhood adversity, the relationship of war exposure to PTSD remains equally strong across all levels of sensitivity (Fig. 3).
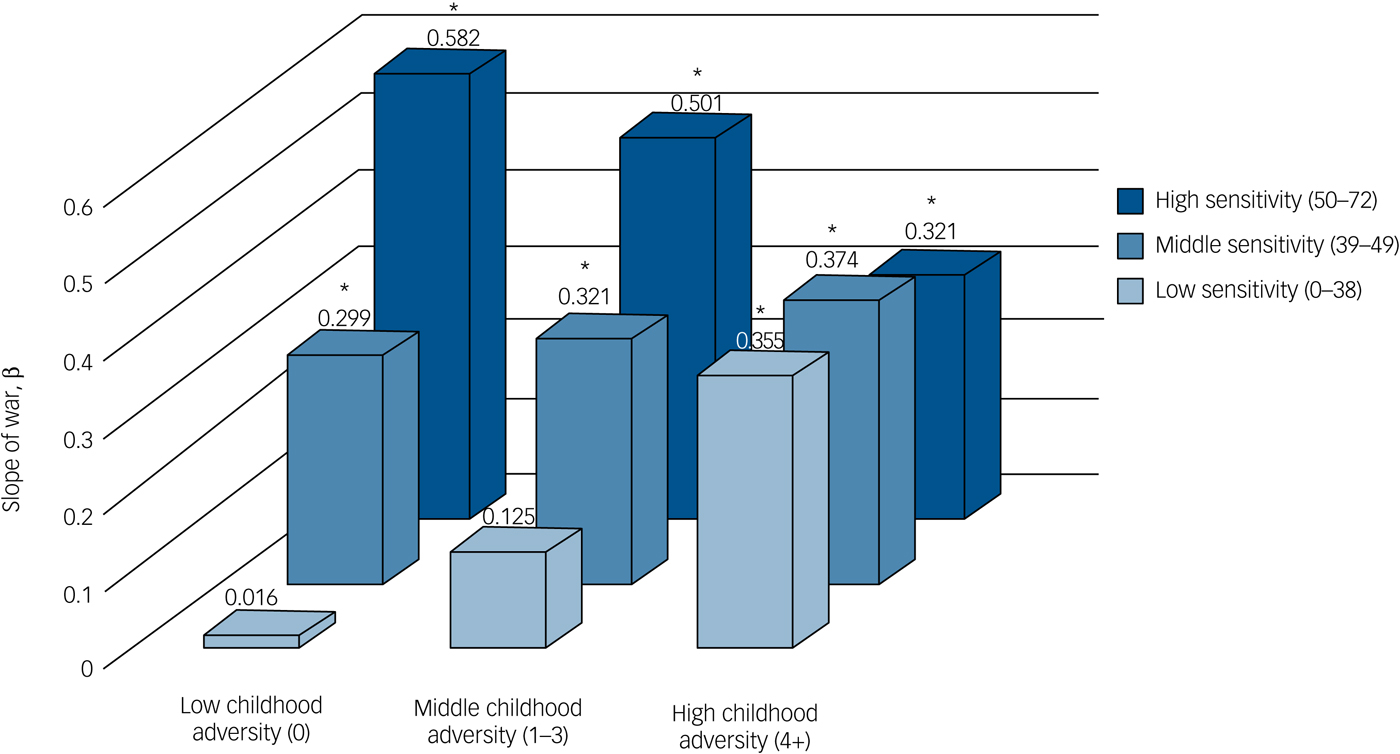
Fig. 3 Relationship of war to post-traumatic stress disorder across varying childhood adversity and sensitivity groups (n = 457).
Discussion
Main findings
War has ravaged Syria since 2011 and is still going on at the time of this writing. There are currently many efforts internationally aimed at the mental health of Syrian refugees. PTSD after war exposure had been classically assessed by focusing on one trauma or set of traumas while neglecting other non-war traumas. The real picture, however, is more complex and traumas do not occur typically in isolation. In this study we assessed PTSD in 549 Syrian refugee children and adolescents who were integrated into the Lebanese public school system and investigated the role of war trauma, childhood adversities as well as personal sensitivity in predicting the final 1-month PTSD picture. A variety of well-established childhood adversities and war traumas were assessed with approximately two-thirds of children and adolescents reporting at least one war trauma and a similar percentage reporting at least one childhood adversity. War events and childhood adversities were positively correlated as we had previously found in a nationally representative sample.Reference Itani, Haddad, Fayyad, Karam and Karam6
Childhood adversities were clearly the most important predictor of PTSD in our sample. Their impact held not only independently but also in interaction with war and sensitivity. The effect of war on PTSD was dependent on the interplay between childhood adversities and sensitivity. Whereas different levels of sensitivity did not predict any differences in PTSD when childhood adversities were high, at low levels of adversities, sensitivity moderated the effects of war on PTSD with more sensitive children being more vulnerable to the effects of war than less sensitive children.
Interpretation of our findings
In more detail, the effects of war on PTSD were strongest in children with high sensitivity and low childhood adversities and weakest in children with low sensitivity and low childhood adversities but at a similar moderate level, regardless of sensitivity differences, when childhood adversities were high. This suggests that sensitivity is an important moderator of the negative effects of war, but only in a developmental context that is relatively free of other chronic adverse conditions such as an unsupportive family environment.
One interpretation of these results is that sensitive refugee children that have not been exposed to other adversities are more vulnerable to the effects of war, possibly because these children have been more sheltered from other adversities. Sensitive children exposed to significant childhood adversities, on the other hand, may have developed coping strategies over time, which make them slightly less vulnerable to the development of PTSD (i.e. stealing effects).Reference Rutter26 Although Okello et al Reference Okello, De Schryver, Musisi, Broekaert and Derluyn10 had not assessed sensitivity, they found in a sample of adolescents attending schools in Northern Uganda that in those with lower levels of childhood adversities, stressful war experiences were more strongly related to PTSD than in adolescents with higher levels of childhood adversities.
There are some studies that have looked at temperament and personality traits in predicting the relationship between trauma or adversities and PTSD.Reference Weems, Pina, Costa, Watts, Taylor and Cannon27–Reference North, Abbacchi and Cloninger29 However, we are not aware of any studies that explored the triangular effect of childhood adversities, sensitivity or other personality features on the final effect of disasters (such as war) on mental health including PTSD. Hence, this is, to our knowledge, the first study to explore the interaction between sensitivity, childhood adversities and war on PTSD in children. The relative roles of childhood adversities and war in predicting PTSD is important not only to assess the relative burden of war but also to properly direct treatment of war-exposed children and their families and possibly to decrease the impact of war in populations at risk.
Limitations
Limitations include the fact that these children were already enrolled in the public school system, and thus may have had more time to adapt in Lebanon and have families with more social means, and thus might not be representative of all Syrian children and adolescents in Lebanon. We did not have information on length of war exposure nor of exposure to adversities. The data we had on the length of time children had lived in Lebanon was limited to a subsample and we were not therefore in a position to consider our findings in relation to time since war exposure.
Another conceivable limitation has to do with not using the PTSD diagnosis categorically. However, it is well established that many children who are exposed to wars and disasters do not show severe PTSD symptoms nor meet criteria for the full PTSD diagnosis. Using the PTSD-RI scores allowed us to measure the severity of symptoms as continuous scores and this is consistent with several studies investigating war-affected children and the outcome of PTSD scores over time.Reference Thabet and Vostanis1, Reference Nader, Pynoos, Fairbanks, Al-Ajeel and Al-Asfour23, Reference Pynoos, Frederick, Nader, Arroyo, Steinberg and Eth30–Reference Wolmer, Laor, Dedeoglu, Siev and Yazgan32
In this paper, only the effect of sensitivity has been considered. A potential limitation is not taking into account other individual or temperament traits that could have played a role. A final limitation may be that the child was the only informant interviewed in our study. However, parents in the context of war may not be fully aware of their children's full exposure to war events and other adversities.
Implications
These findings lead to several practical conclusions with relevance to public health and planning of interventions. Although it seems logical that non-war traumas play a major role in the mental health of refugees, nonetheless these findings point to the importance of assessing comprehensively the traumatic picture in refugees. Not only do they co-occur, but they are positively related (the more childhood adversities the more war traumas). The ‘more sheltered’ children and adolescents are more likely to suffer heavily, especially if highly sensitive. These findings have direct relevance to non-governmental organisations and frontline personnel trying to identify which war-exposed children need intervention: screening for childhood adversities is of paramount importance in order to offer targeted family and peer-group interventions as well.




eLetters
No eLetters have been published for this article.