



Overconsumption of food products with high sugar content contributes to an unhealthy diet. Excessive sugar consumption not only increases overall energy intake but is also often associated with a lower intake of more nutritionally adequate energy content, which may result in multiple negative health outcomes (e.g., weight gain, diabetes, dental diseases(1)). Several health authorities have already issued recommendations regarding the intake of free or added sugars (for a review, see (Reference Mela and Woolner2)). For instance, the WHO issued guidelines for the intake of free sugars (i.e., ‘… monosaccharides and disaccharides added to foods and beverages by the manufacturer, cook or consumer and sugars naturally present in honey, syrups, fruit juices and fruit juice concentrates’), stating that it should be limited to <10 % (ideally 5 %) of the total daily energy intake(1). To illustrate, for a person with a 2000 kcal/daily intake, free sugars intake should be <50 g (or about twelve teaspoons)/d.
A recent review of representative surveys across eleven European countries found that added sugars represent between 7·3 % (in Norway) and 11·4 % (in the UK) of adults’ energy intake(Reference Azaïs-Braesco, Sluik and Maillot3). For children and teens, these numbers are even higher (from 11 % in Denmark to 16·8 % in the Netherlands). According to the National Food, Nutrition and Physical Activity Survey(Reference Lopes, Torres and Oliveira4,Reference Lopes, Torres and Oliveira5) , in Portugal, free sugars contribute on average to 7·5 % of total daily energy intake (9·6 % for children and 10·5 % for teens). Moreover, the results showed a high prevalence of excessive consumption of free sugars (i.e., above 10 % of total energy intake) for the overall population (24·3 %), for children (40·7 %) and for teens (48·7 %), suggesting an imperative need to address this problem.
Reducing population intake of free sugars is a complex issue that requires government action, along with the engagement of other parties of the food system such as the production industry, retailers, hospitality sector, as well the media(Reference Evans6). Change may be attained by implementing strategies such as population education (e.g., national dietary guidelines), point-of-purchasing labelling (e.g., food package nutrition fact panels), fiscal (dis)incentives (e.g., soft drinks taxes), industry quality standards (e.g., mandatory or recommended limits for sugar, trans fat, etc.) and food marketing standards (e.g., limited marketing towards children of products that fail to meet nutrition standards(Reference Mozaffarian, Angell and Lang7,Reference Popkin and Hawkes8) ).
We are particularly interested in examining how individuals perceive and accept governmental interventions aimed at reducing sugar intake. Assessing public perception is relevant because public has shown to be a key enabler for political action, as decision-makers respond favourably to issues supported by their electorates(Reference Cullerton, Donnet and Lee9,Reference Cullerton, Donnet and Lee10) . Moreover, public perception also potentially shapes the design, implementation and compliance with a given policy (e.g., (Reference Reynolds, Archer and Pilling11)). Next, we briefly present an overview of the governmental measures that have been developed in the Portuguese context.
Current governmental interventions aimed at reducing sugar intake in Portugal
In 2016, the Portuguese government developed a public health programme aiming, among other goals, to prevent diabetes and obesity through the promotion of health literacy(12). Besides this focus on promoting citizens’ capability to make informed choices about their health, multiple actions have also been implemented to promote healthier dietary habits (for a review, see (Reference Graça, Gregório and de Sousa13)). For example, to reduce the excessive intake of sugar, salt and fat, there is a regulation defining which products may be sold in vending machines placed in national healthcare facilities(14). This regulation was subsequently generalised to the products sold (or advertised) in cafeterias placed in these facilities(15). For instance, whereas some products are forbidden (e.g., cakes, pastry, soft drinks), others can be allowed if complying with guidelines regarding composition (e.g., cookies with up to 20 % of sugar content) or portion sizes (e.g., chocolates without filling may be available in portions up to 50 g).
Another action that illustrates an environmental intervention to facilitate healthier choices is the reduction of the weight of individual sugar packets. These packets usually contained 8 g of sugar and were reduced to 5/6 g via an agreement between the ministry of health and food industry representatives(16). A revised agreement defines that in 2020 single-serve packets should contain up to 4 g of sugar. Regarding population-based information campaigns, a recent 2018 advertisement, disseminated on TV and social media, aimed to raise awareness about hidden sugars.
Increased taxation on sugar-sweetened beverages (SSB) was approved in the state budget in 2017 (i.e., each hectolitre of non-alcoholic beverages up to 80 g of sugar/l was taxed by €8·22, and the taxation roughly doubled for beverages exceeding that amount of sugar(17)). Although these taxes were essentially maintained in the state budget for 2018(18), they were extensively reviewed for 2019(19), further encouraging the reduction of sugar content.
Given that these interventions are recent, there is still, to our knowledge, no available information regarding their impact. An exception refers to the impact of taxation, with preliminary data suggesting a 11 % reduction of the total energy intake through SSB consumption(Reference Goiana-da-Silva, Cruz-e-Silva and Gregório20,Reference Goiana-da-Silva, Nunes and Miraldo21) . This pattern is in line with previous results in other countries showing that these types of fiscal measures have been effective in promoting reduced sugar intake(Reference Thow, Downs and Jan22).
Consumer acceptance of interventions to regulate sugar intake elsewhere
Several studies have examined how individuals evaluate policy interventions aimed at changing various behaviours, such as tobacco and alcohol use, as well as diet and physical activity (for a review, see (Reference Diepeveen, Ling and Suhrcke23)). We will focus on interventions designed to improve diet quality. For example, a study found that British participants highly supported policies for weight management such as healthy lifestyle campaigns and food labelling (i.e., fat and energy content of foods in restaurants), but not taxation of unhealthy foods(Reference Beeken and Wardle24). Another study showed that Australian participants agreed with government-driven actions to address overweight and obesity rates, with interventions restricting the advertisement of unhealthful food to children and to a lower extent with fiscal actions(Reference Sainsbury, Hendy and Magnusson25). A recent study(Reference Cadario and Chandon26) also examined the acceptance level of various healthy eating nudges for American consumers and found that descriptive nutritional labelling obtained the highest approval. Overall, as suggested by a survey including five European countries, the more intrusive the intervention (e.g., bans or taxations), the lower the support(Reference Mazzocchi, Cagnone and Bech-Larsen27). Likewise, another cross-national study with six European countries showed that the least intrusive interventions (i.e., those that entail information provision by the government) were supported across countries(Reference Reisch, Sunstein and Gwozdz28). However, significant differences emerged for the overall approval of the total set of nine interventions (e.g., around 74 % support was found in Italy, the UK and France, followed by Germany with 69 % and then by Hungary and Denmark with 57·1 and 54 %, respectively).
Although some inferences may be drawn from these studies, research specifically focusing on how consumers perceive (and react to) different governmental interventions to reduce sugar intake is still scarce. Some studies have taken a qualitative approach to this issue. For instance, a study analysing the content of American press coverage of the SSB taxation debate found mainly pro-taxation arguments (e.g., health and financial benefits of taxation(Reference Niederdeppe, Gollust and Jarlenski29)). More recently, an examination of public responses to an SSB tax proposal in the UK (i.e., readers’ comments to online news covering this intervention) showed that consumers perceived this measure as a challenge to the autonomy of individuals who should be responsible for their own diet. Mistrust in the authorities (e.g., government, industry, public health experts) also emerged, namely regarding the true purpose of the tax (i.e., raise revenue instead of reducing sugar intake) or of alternatives (i.e., replacing sugar by artificial sweeteners(Reference Thomas-Meyer, Mytton and Adams30)).
We identified two important contributions focused on the public acceptance of a set of government interventions aimed at reducing sugar intake. First, a study by Petrescu et al. (Reference Petrescu, Hollands and Couturier31) compared how British and American participants rated the acceptability of five interventions aimed at reducing the intake of SSB. Consumer education was rated as the most acceptable and taxation the least acceptable strategy. No overall differences were found according to country, with the exception that British participants were more in favour of reducing portion sizes. The second important contribution is provided by the study by Hagmann et al. (Reference Hagmann, Siegrist and Hartmann32) that included a large sample of Swiss participants. Specifically, participants were asked to rate their agreement, using seven-point rating scales, with the implementation of eight strategies, including public health campaigns, reducing sugar content in products or replacing sugar with artificial sweeteners or nudging (e.g., reducing the availability of foods containing high sugar content). Overall, participants agreed with most interventions, particularly with the labelling of sugar content, followed by public health campaigns. Only three interventions were rated below the agreement scale midpoint: restriction of portion sizes of foods high in sugar, taxation and replacing sugar in specific food categories (breakfast cereals and yogurt) by artificial sweeteners.
In the current work, we examined public acceptance of different interventions aimed at reducing sugar intake in Portugal. To our knowledge, Portugal was not included in previous studies examining the acceptance of interventions promoting healthy eating in general(Reference Mazzocchi, Cagnone and Bech-Larsen27,Reference Reisch, Sunstein and Gwozdz28) , or reduction of sugar intake in particular(Reference Petrescu, Hollands and Couturier31,Reference Hagmann, Siegrist and Hartmann32) . To that end, we assessed the agreement level with the set of sugar reduction interventions described in Hagmann et al.’s study(Reference Hagmann, Siegrist and Hartmann32). In addition to identifying which interventions received greater support, we explored how the overall acceptance of the interventions is shaped by variables related to sugar consumption (e.g., consciousness of sugar intake, frequency of sugary products consumption) as well as by individual characteristics. For instance, individuals who pay more attention to their sugar intake also show greater support of interventions(Reference Hagmann, Siegrist and Hartmann32). Previous research has also shown that higher acceptance may be found among women(Reference Diepeveen, Ling and Suhrcke23,Reference Sainsbury, Hendy and Magnusson25,Reference Reisch, Sunstein and Gwozdz28,Reference Hagmann, Siegrist and Hartmann32) , older participants(Reference Diepeveen, Ling and Suhrcke23), participants with tertiary education(Reference Sainsbury, Hendy and Magnusson25) and those with children(Reference Sainsbury, Hendy and Magnusson25). Moreover, we also assessed the extent to which consumers perceived reducing sugar intake in the Portuguese population as an important and urgent issue and which age groups should be prioritised.
To the extent that Portuguese health authorities have recently implemented several actions (e.g., taxation, restrictions on foods and beverages available in healthcare facilities), we also aimed to explore which of these interventions were more salient to the participants. Specifically, just prior to the acceptance ratings, we included a free-recall task to examine whether participants were aware and remembered the Portuguese government actions intended to reduce sugar intake.
Method
Participants
The current study included 1010 Portuguese volunteers (76·7 % female, 22·9 % male and 0·4 % other) aged between 18 and 82 years (M 36·33 years, sd 13·22). Most of the participants reported having at least a college degree (78·8 %), to be employed (77·5 %), to be in a cohabiting romantic relationship (50·0 %) and not having children in the household (66·5 %). Moreover, most participants reported following a regular omnivorous diet (72·5 %) and a BMI within the normal weight range (i.e., 18·5–24·9, 58·5 %).
Instruments and procedure
Participants were invited, through an institutional email and social networks, to collaborate on a web survey about food habits. When clicking on the provided link, they were directed to a secure webpage hosted in Qualtrics containing information about the goals of the study, its expected duration (approximately 15 min) and ethical considerations (i.e., anonymity, confidentiality and the possibility to withdraw from the study at any point). The only incentive to participate was the opportunity to win one of the three commercial vouchers (€50). The survey was administered in European Portuguese, and participation was restricted to Portuguese adults. After agreeing to collaborate in the study, participants were presented with a set of socio-demographic questions (e.g., sex, age, level of education, number of children in the household) and with the main study variables. As the survey was part of a broader project, we will only describe the relevant measures for the current paper.
First, participants responded to an item assessing sugar consciousness (Reference Hagmann, Siegrist and Hartmann32) (i.e., How much attention do you pay to the sugar content in your diet?, from 1 = Not at all to 7 = Very much). Next, participants indicated their general frequency of consumption of foods and beverages with high sugar content by selecting one of the seven options (from 1 = Never or less than once a month to 7 = More than once a day). Participants were then asked about their attitudes towards reducing sugar intake in the Portuguese population using two rating scales: ‘In your opinion, reducing sugar intake for the Portuguese population is…’ (i) from 1 = Not very important to 7 = Very important and (ii) from 1 = Not very urgent to 7 = Very urgent. Both items were positively and strongly correlated, r 0·73, p < 0·001, and were combined into a single index.
Subsequently, a free-recall task regarding interventions aimed at reducing sugar intake was introduced. Specifically, participants were asked ‘Do you recall any official intervention or policy aimed at reducing sugar intake in the Portuguese population?’ (Yes/No). Participants who selected ‘yes’ were asked to list and describe, in their own words, all the interventions they could remember.
After this task, we assessed their general acceptance of interventions to reduce sugar consumption by adapting the instrument from Hagmann et al. (Reference Hagmann, Siegrist and Hartmann32) to European Portuguese. Across items, we replaced the expression ‘foods high in sugar’ for ‘products high in sugar’ to include both foods and beverages. Participants were asked ‘Please indicate to what extent do you agree with each of the following governmental strategies aimed at reducing sugar intake in the Portuguese population’ using seven-point rating scales (from 1 = Do not agree at all to 7 = Fully agree). Specifically, the eight items were related to (i) reducing the availability of high sugary products (‘The availability of products containing high levels of sugar should be reduced’ (e.g., no sales at vending machines)), (ii) taxation (‘Increased taxation should be applied to products with high sugar content’), (iii) advertisement ban (‘Advertisements for products high in sugar should be forbidden’), (iv) reducing portion size (‘There should be a limit of the portion size of foods high in sugar’), (v) labelling (‘The sugar content should be clearly visible on a label on the package of products high in sugar’), (vi) sugar reduction in products (‘There should regulations for the food industry about the maximum amount of sugar that products may contain’), (vii) substitution of sugar by artificial sweeteners (‘Sugar in products should be replaced by artificial sweeteners’) and (viii) public health campaigns (e.g., ‘Population-based information campaigns promoting a reduction of sugar content in the diet should be conducted’). This scale presented an acceptable reliability in the current study (α = 0·77).
Finally, participants were asked to indicate how important (from 1 = Not very important to 7 = Very important) would be to reduce sugar intake in five age-groups (i.e., ‘children up to 6 years old’, ‘children from 6 to 12 years old’, ‘teenagers’, ‘adults’ and ‘elderly’; α = 0·84).
At the end of the survey, participants were asked additional control measures, namely to indicate their diet(s) type(s), height and weight (open-ended answers, including ‘I don’t know/I rather not say’ options), and finally asked to rate their overall health status (from 1 = Very bad to 7 = Very good (Reference Gréa Krause, Beer-Borst and Sommerhalder33)).
Results
Only completed questionnaires were retained, and statistical analyses were performed using IBM SPSS Statistics version 25.
Interventions: free-recall task
Results showed that 649 (64·3 %) participants did not remember any specific intervention aimed at reducing sugar intake in the Portuguese population, whereas 361 (35·7 %) participants indicated remembering such interventions. However, forty-six did not indicate any specific measure. The remaining 315 participants indicated between one and four interventions (M 1·35, sd 0·58), in a total of 425 interventions. Responses were then discussed and categorised by three independent judges. Results are summarised in Table 1, including examples of participants’ responses per category.
Table 1 Categorisation of recalled interventions aimed at reducing sugar intake*

* Percentages calculated based on the total number of interventions.
† Results refer to the frequencies of sub-categories in relation to the total frequency of the category.
As shown in Table 1, the most frequently mentioned intervention was increasing prices or taxation for products with high sugar content, particularly for soft drinks, followed by the reduction of the quantity of sugar in individual sugar packets. The third most frequent intervention was related to the limited availability of products with high sugar content in healthcare or education facilities, either in vending machines or in cafeterias. Less than 10 % of the interventions mentioned were related to raising public awareness or promoting consumer knowledge about sugar.
Descriptive results and correlations
As shown in Table 2, overall, participants supported the interventions, considered important reducing sugar intake across age groups and had positive attitudes towards sugar intake reduction in Portugal. They also reported paying attention to sugar intake in their own diet, to ingesting sugar less frequently and to be in good general health.
Table 2 Overall descriptive results (M, sd, CI) and correlations†
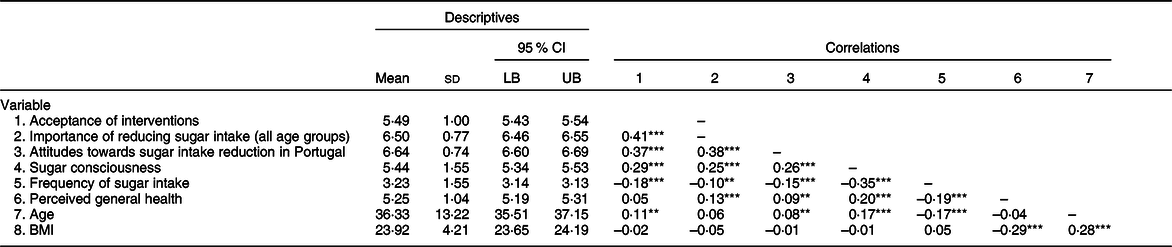
LB, lower bound of the confidence interval; UB, upper bound of the confidence interval.
**p < 0·010, ***p < 0·001.
† All variables refer to the full sample (n 1010), except for BMI due to missing values in height or weight (n 951).
Correlations between study variables are also presented in Table 2. Overall, the acceptance of interventions designed to reduce sugar intake was positively correlated with the ratings of importance of reducing sugar intake across all age groups, p < 0·001 and positive attitudes towards sugar reduction for the Portuguese population in general, p < 0·001. These latter two variables were also positively correlated, p < 0·001. Moreover, we also observed positive associations between these three variables with sugar consciousness, all p’s < 0·001 and negative associations with the self-reported frequency of consumption of high sugary foods and drinks, all p’s ≤ 0·001. Self-reported general health was also positively correlated with ratings of importance of reducing sugar intake across all age groups, p < 0·001, and attitudes towards reduction for the Portuguese population in general, p = 0·004. BMI was only positively associated with age, p < 0·001, and negatively associated with perceived general health, p < 0·001.
Acceptance of interventions designed to reduce sugar intake
For all interventions, acceptance ratings varied between 1 and 7. The repeated measures ANOVA (with Huynh–Feldt correction, as sphericity assumption was not verified) showed that the level of acceptance differed significantly between interventions, F(5·185, 230·22) = 605·32, MSE = 1492·85, p < 0·001, η 2 p = 0·38. Post hoc tests with Bonferroni correction showed significant differences between all strategies, all p’s < 0·046, except between ‘reducing availability’ and ‘sugar reduction in products’.
Overall, participants reported accepting all interventions (see Table 3), with the exception of replacing sugar in food products by artificial sweeteners, which obtained the lowest acceptance level. The most accepted intervention was the one related to sugar labelling (i.e., ‘The sugar content should be clearly visible on a label on the package of foods high in sugar’).
Table 3 Acceptance ratings for different interventions (overall sample)*
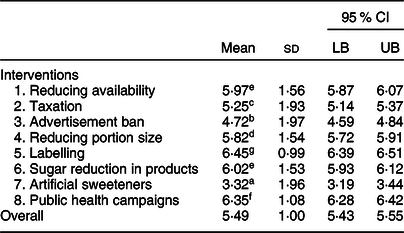
* Different superscripts (a–g) indicate different levels of acceptance between interventions.
Sex differences in the acceptance of the interventions are shown in Fig. 1. Women (v. men) showed higher acceptance for most interventions, all p’s < 0·027. Still, no significant sex differences were found for taxation t(1004) = 1·80, p = 0·080, d = 0·11, advertisement ban, t(1004) = 1·88, p = 0·066, d = 0·12, and artificial sweeteners, t < 1.

Fig. 1 Sex differences in the acceptance of the interventions. Results for multiple comparisons are corrected using 5000 bootstrap samples. Error bars represent se. *p < 0·05, **p < 0·01, ***p < 0·001. ![]() , men;
, men; ![]() , women
, women
Overall, no differences were detected according to the level of education, all p’s ≥ 0·260, except for one intervention: participants with higher education reported greater support for the taxation of high sugar products (M 5·37, sd 1·83) than those with lower levels of education (M 4·83, sd 2·20), t(298·77) = 3·28, p = 0·001, d = 0·34. We also found that participants with (v. without) children in the household agreed more with the advertisement ban, t(1008) = 2·07, p = 0·038, d = 0·13. No other differences were detected, all p’s ≥ 0·164.
Age was positively (but weakly) correlated with the acceptance of the following interventions: advertisement ban (r 0·21, p < 0·001), labelling (r 0·07, p = 0·027), sugar reduction in products (r 0·09, p = 0·004) and public health campaigns (r 0·11, p = 0·001). In contrast, age was negatively associated with the acceptance of replacing sugar by artificial sweeteners, r –0·06, p = 0·044. Finally, we did not find overall differences according to BMI. The only difference that approached conventional levels of significance was that overweight (v. non-overweight) participants tended to be more supportive of replacing sugar by artificial sweeteners, t(585·11) = 1·97, p = 0·052, d = 0·16, all other p’s ≥ 0·229.
Prioritised age-groups for sugar reduction
The repeated measures ANOVA (with Huynh–Feldt correction, as sphericity assumption was not verified) showed that the perceived importance of reducing sugar consumption varied according to target age group, F(2·642, 665·84) = 80·39, MSE = 56·21, p < 0·001, η 2 p = 0·14. Results are summarised in Table 4. Although participants evaluated the reduction of sugar consumption across age groups as highly important, post hoc tests with Bonferroni correction showed that adults were the least prioritised age group, all p’s < 0·021, followed by the elderly (but not different from teenagers, p = 0·177). The most prioritised target group for reducing sugar intake was children irrespective of their age (i.e., up to 12 years old), p = 0·134.
Table 4 Importance of sugar intake reduction for different age groups (overall sample and according to sex)*
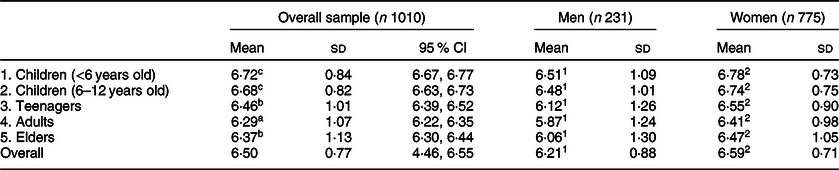
* Different superscripts (a–g) indicate differences in the perceived importance of reducing sugar intake according to age groups and different superscripts (1 and 2) indicate sex differences.
As shown in Table 4, women (v. men) considered more important to reduce sugar intake across age groups, all p’s ≤ 0·002. We also found that participants with children (v. without) in the household considered more important to reduce sugar intake for children, either up to 6 years old, t(980·61) = 3·20, p = 0·001, d = 0·20, or up to 12 years old, t(877·92) = 2·55, p = 0.009, d = 0·17. For teenagers, this sex difference was only marginal, t(740·23) = 1·92, p = 0·057, d = 0·10, and no differences were observed for the other age groups, all p’s ≥ 0·279.
Hierarchical regression analysis
Table 5 presents the results of the hierarchical regression with general acceptance of interventions as the outcome variable. In each block, we entered individual characteristics (step 1) and variables related to sugar consumption (step 2). The final model was significant, F(8, 997) = 41·88, MSE = 31·40, p < 0·001, and explained 25 % of the variance on interventions’ acceptance.
Table 5 Hierarchical regression analysis: general acceptance of interventions designed to reduce sugar intake
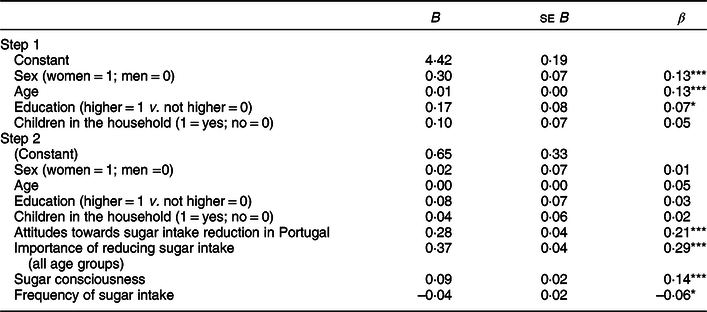
R 2 = 0·25; *p < 0·050, **p < 0·010, ***p < 0·001.
As shown in Table 5, the results of step 1 indicate that general acceptance of the interventions were significantly associated with sex (p < 0·001), age (p < 0·001) and education (p = 0·034), such that higher support was found for women, older participants and those with higher education. Having children in the household was unrelated with the overall acceptance of interventions, p = 0·151. However, the inclusion of variables related to sugar consumption in step 2 rendered the associations of individual characteristics non-significant. Instead, we found that general acceptance of the interventions was more strongly associated with the perceived importance of reducing sugar intake, attitudes towards reducing sugar intake in Portugal, and by sugar consciousness, all p’s < 0·001.
Discussion
Governments worldwide have been implementing policies aiming to improve citizens’ health, by discouraging some behaviours (alcohol or tobacco consumption) and encouraging others (exercising, healthier eating). In a recent WHO report, most countries reported having nutrition-relevant policies(34). However, despite this progress, we are far from attaining the goals set in the Global Action Plan for the prevention and control of non-communicable diseases(35), particularly those related to obesity and diabetes. Assessing how individuals perceive such interventions is crucial for different stages of policymaking, from the build-up of political will for governments to take action to the evaluation of their efficacy(Reference Reynolds, Archer and Pilling11). Previous research suggested that the more intrusive the intervention, the least acceptance it will receive(Reference Cadario and Chandon26–Reference Reisch, Sunstein and Gwozdz28,Reference Petrescu, Hollands and Couturier31) . We focused on interventions aimed at reducing sugar intake, which is still an understudied topic. Portugal offers an interesting context to study this issue because, due to the high sugar intake, several policies have been implemented in recent years(Reference Graça, Gregório and de Sousa13).
Hagmann et al. (Reference Hagmann, Siegrist and Hartmann32) found support for most interventions aimed at reducing sugar intake, except for reducing portion sizes, taxation and replacing sugar by artificial sweeteners. Our findings were slightly different as participants were highly supportive of all interventions, except the one related to artificial sweeteners. Still, both studies concur on the most and least supported interventions – labelling of sugar content and replacement of sugar by artificial sweeteners, respectively. Strategies aimed at informing consumers such as nutritional labelling have also obtained the highest levels of approval in other studies(Reference Cadario and Chandon26). The lack of support for sugar substitution by artificial sweeteners is also not surprising, as consumers seem to mistrust the use of food additives, considering them less natural, unhealthy and related to negative health outcomes (for a review, see (Reference Szűcs, Szabó and Guerrero36)). Still, results from Hagmann et al. (Reference Hagmann, Siegrist and Hartmann32) suggested that some consumers, namely overweight individuals, may be more supportive of interventions focused on the substitution of sugar by artificial sweeteners. Although this type of sweeteners has been marketed as a healthier alternative to sugar intake, the debate about its benefits is still ongoing. For instance, it has been suggested that while it may contribute to weight reduction(Reference Laviada-Molina, Molina-Segui and Pérez-Gaxiola37), some important safety issues have also been detected(Reference Purohit and Mishra38,Reference Kakleas, Christodouli and Karavanaki39) . Overall, because the intake of sweeteners has not been consistently associated with health benefits, some dietary guidelines (e.g., in Canada(40)) proposed that the intake of free sugars should be achieved through the promotion of unsweetened beverages instead.
We also examined how the acceptance of specific interventions may vary according to individual characteristics. In line with other studies, age and sex differences emerged for most interventions, with older participants and women showing higher acceptance overall(Reference Sainsbury, Hendy and Magnusson25,Reference Hagmann, Siegrist and Hartmann32) . Regarding education level and presence of children in the household, the results were restricted to specific interventions, such that highly educated participants were more in favour of taxation, whereas participants with children in the household were more in favour of advertisement ban for products high in sugar. However, we did not find differences in the acceptance of the intervention according to BMI(Reference Hagmann, Siegrist and Hartmann32).
Participants also reported positive attitudes towards the need of reducing sugar intake in the Portuguese population and agreed with the importance of reducing sugar intake across all age groups, particularly among children. Likewise, participants indicated paying attention to the amount of sugar they consume, which was also in line with a low self-reported frequency of consumption of high sugary foods and beverages. Importantly, results from a hierarchical regression analysis showed that all these variables were significantly associated with the acceptance of interventions, particularly attitudes towards the need of reducing sugar intake in Portugal and perceived importance of reducing sugar intake across age groups, over and above social-demographic variables (i.e., age, education and sex). In fact, these results were found independently of any a priori difference according to individual characteristics.
Another important contribution of the current work is the demonstration of which interventions implemented in Portugal are most salient to participants. Although only about one-third of the participants could remember at least one intervention, we still obtained 425 intervention descriptions. The most frequently mentioned interventions were those related to increased prices or taxation for products (particularly beverages) with high sugar content, reduction in the weight of individual sugar packets and limited availability of products offered in healthcare or education facilities. Both the taxation and interventions limiting the availability of sugary products have been recently legislated and implemented in Portugal, whereas the reduction of the individual sugar packets stems from an agreement between health authorities and an association representing the hospitality industry. We can speculate that the salience of this latter intervention may be explained by its pervasiveness in everyday life, due to the Portuguese high coffee consumption patterns. Future studies should seek to further explore the information sources regarding these interventions (i.e., press, social media), as well as their perceived impact in consumers shopping and consumption behaviours, including individual strategies to reduce sugar intake (for a review, see (Reference Rodda, Booth and Brittain41)). The labelling of sugar content was spontaneously mentioned by <2 % of respondents which was surprising given that it received the highest acceptance rating.
In general, our results suggest an optimistic scenario both from a policymaking and a public health standpoints, as our participants were very receptive to the implementation of interventions aimed at reducing sugar intake, reported positive attitudes towards the need of addressing excessive sugar intake and were already paying attention to their own sugar intake. However, we recommend caution in the generalisation of the results to the Portuguese population, as it is possible that this high support is related to specific characteristics of the volunteers who participated in the current study. A participation bias in nutrition-related studies is not uncommon (e.g., women and highly educated individuals are more likely to participate in this type of research(Reference Andreeva, Salanave and Castetbon42)). Indeed, our sample differs from the overall population regarding the level of education and BMI. Specifically, our sample is highly educated (almost 80 % with higher education), whereas the proportion of population (25–64 years old) with tertiary education in Portugal is only 25 %(43). The fact that participants were recruited through a university may have also contributed to such differences in the level of education. Also, almost 60 % of our sample reported a BMI within the normal weight range, which differs from the 43 % found in the overall Portuguese population (although close to the 56·1 % found for population with higher education(Reference Lopes, Torres and Oliveira5)). Noteworthy, these results do not provide any evidence regarding the association between the acceptance of a given intervention and its efficacy. For example, a recent study(Reference Cadario and Chandon26) found that although approval for healthy eating interventions was positively associated with perceived effectiveness, it was negatively associated with actual effectiveness. Furthermore, the available evidence regarding the efficacy of interventions aimed at reducing sugar intake is mostly focused on the consumption of specific products (e.g., SSB) or interventions (e.g., taxation(Reference Kirkpatrick, Raffoul and Maynard44)). Therefore, more studies are needed to assess how the implementation of such interventions may contribute to actual healthier food choices.
Another potential limitation of the current study is that most items included broad descriptions of the interventions in terms of the target population, or even the product categories they refer to. Concerning the latter, all the items referred to products with high sugar content in order to include both foods and beverages. However, it is possible that acceptance might differ if the items are framed for SSB or specific food categories. Indeed, policies have prioritised the reduction of SSB intake(Reference Popkin and Hawkes8), namely through taxation(Reference Hagenaars, Jeurissen and Klazinga45). Consumers may be more prone to accept such interventions, as these types of beverages constitute examples of products consistently perceived as unhealthy. Regarding the target population of interventions, previous studies have shown that individuals are particularly supportive of interventions targeting children(Reference Sainsbury, Hendy and Magnusson25), which may be important when determining their acceptance. For example, we observed that, although participants are in favour of advertisement ban intervention, this was the second least supported intervention. However, such acceptance level was likely to increase if the ban was directed at products marketed for children (which was actually issued in Portugal very recently)(46). Future studies could also consider including more items to measure acceptability(Reference Petrescu, Hollands and Couturier31), as well as assessing related constructs (e.g., beliefs about the causes of obesity, considering that people who attribute obesity to the food environment tend to be more supportive of policy interventions(Reference Beeken and Wardle24)). Another suggestion concerns the inclusion of more detailed measures of frequency of consumption of high sugar foods and beverages, as well as the contexts in which they are consumed.
Intervention acceptance is a crucial issue to consider when planning future policy interventions, and despite the general public being a key audience to assess in this regard, it may also be important to include other stakeholders, such as healthcare professionals, behaviour change experts and politicians. In addition, aspects other than acceptance, such as financial viability, effectiveness, equity and potential side-effects, are also essential to consider when designing and planning the implementation of such policies(Reference Michie, Atkins and West47).
The current study identifies which interventions aimed at reducing sugar intake had higher visibility (as suggested by the free-recall task) and acceptance levels in Portugal. Still, due to the high complexity of the food consumption patterns, it is unlikely that the implementation of one type of intervention alone will suffice to address the issue. Indeed, multiple interventions need to be implemented simultaneously(Reference Thow, Downs and Jan22) with the aim of contributing to changes in the food culture(Reference Evans6). Moreover, although policies focusing on a single aspect are useful for the reduction of specific additives (e.g., added sugar), they can also be reductionist as they do not focus on overall diet quality(Reference Mozaffarian, Rosenberg and Uauy48). Hence, comprehensive policies are needed to address the high levels of sugar intake and foster healthy eating behaviours among populations. Knowledge on how people perceive and accept different interventions for the reduction of sugar intake is an important step towards that end and is vital to support government action in this area.
Acknowledgements
Acknowledgements: The authors would like to thank Hugo Pais for his help in data collection. Financial support: The current research was financially supported by Project LISBOA-01-0145-FEDER-028008, co-funded by the Lisboa 2020 programme, Portugal 2020, and European Union through FEDER (Fundo Europeu de Desenvolvimento Regional/ European Regional Development Fund) funds and by national funds through the Foundation for Science and Technology. Conflict of interest: There are no conflicts of interest to declare. Authorship: Formulation of the research questions and study design: all authors; Data collection: M.P. and C.A.G.; Data analyses: M.P. and D.L.R.; Writing the article: all authors. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Ethics Committee of Instituto Universitário de Lisboa (ISCTE-IUL, approval no. 22/2019). Written informed consent was obtained from all participants.






