


The Mediterranean dietary pattern (MDP) was identified in the olive-growing areas of the Mediterranean region in the late 1950s(Reference Keys and Grande1). The MDP can be defined as a dietary pattern with a high intake of vegetables, legumes, fruits and nuts, cereals (largely unrefined in the past), a high intake of olive oil but a low intake of saturated lipids, a moderately high intake of fish (depending on proximity to the sea), a low-to-moderate intake of dairy products (mostly in the form of cheese or yoghurt), a low intake of meat and poultry, and a regular but moderate intake of ethanol, primarily in the form of wine and generally during meals(Reference Trichopoulou and Vasilopoulou2–Reference Trichopoulou4).
Latest indicators show that the Mediterranean diet is tending to disappear in the Mediterranean area; the Western diet is progressively being implanted instead of the Mediterranean diet; and the nutrition transition, which reflects a progressive alteration in traditional eating and physical activity practices that is associated with the changing demographic and economic profile of countries, is a growing trend in the dietary intake of the Mediterranean countries(Reference Moreno, Sarria and Popkin5–Reference Elmadfa and Weichselbaum12).
The nutrition transition has progressed over lengthy time frames, and focused on subtle shifts in diet and activity patterns, from a starchy, low-variety, low-fat, high-fibre-food diet and labour-intensive work and leisure physical activities to a high-saturated-fat, high-sugar, refined-and-processed foods and low-fibre diet and low physical work and leisure physical activities, which is often termed the ‘Western diet’(Reference Popkin13). The nutrition transition is related to the trends in population health and increased obesity and non-communicable chronic diseases as the primary causes of morbidity and mortality throughout the world(Reference Popkin6).
There are numerous indications that adoption of a Mediterranean diet is associated with increased longevity, decreased morbidity and mortality from CVD, some cancers, obesity, type 2 diabetes and other nutrition-related diseases, and improvements in levels of cardiovascular risk factors(Reference Moreno, Sarria and Popkin5, Reference Corpet and Gerber14–Reference Schroder, Marrugat, Vila, Covas and Elosua24). However, the present prevalence of overweight and obesity in the Mediterranean countries is already considerable, particularly in children(Reference Elmadfa and Weichselbaum12); CVD are the leading cause of death, with cancer as the second most prevalent cause in adults(Reference Elmadfa and Weichselbaum12); and the prevalence of type 2 diabetes is 7·1 % in Italy, 6·1 % in Spain, 5·9 % in Greece, 5·4 % in Portugal and 4·0 % in France(Reference Elmadfa and Weichselbaum12, 25).
Since the Mediterranean diet has long been associated with better health status, several types of Mediterranean dietary score that attempt to evaluate the level of adherence to the MDP have been proposed(Reference Trichopoulou, Kouris-Blazos, Wahlqvist, Gnardellis, Lagiou, Polychronopoulos, Vassilakou, Lipworth and Trichopoulos26–Reference Tur, Romaguera and Pons28). Moreover, several of these indices have been associated with cardiovascular risk factors and biological markers of illness(Reference Panagiotakos, Milias, Pitsavos and Stefanadis29, Reference Panagiotakos, Pitsavos, Arvaniti and Stefanadis30), and it has been shown that maximum adherence to the Mediterranean diet (high Mediterranean dietary score) is associated with the lowest cardiovascular risk factors and with the highest longevity(Reference Trichopoulou, Costacou, Bamia and Trichopoulos16, Reference Esposito, Marfella, Ciotola, Di Palo, Giugliano, D’Armiento, D’Andrea and Giugliano21, Reference Stampfer, Colditz, Willett, Speizer and Hennekens31, Reference Rimm, Giovannucci, Willett, Colditz, Ascherio, Rosner and Stampfer32).
Because of reduced size and isolation due to naturally defined borders, insular environments seem appropriate for bringing to light food habits preserved from external influences, a priori less numerous than on a continent(Reference Tessier and Gerber11). The Greek islands (Greece) and the Balearic Islands (Spain) are located on the two extremes of the Mediterranean Sea. Since the second half of the 20th century, these islands have been important tourist destinations for Europeans(33). The integration of these islands on tourist routes has improved living standards, but also the changes generated by socio-economic development, such as tourism, migration and enhanced commercial availability, are expected to lead to an evolution in food habits by promoting the nutrition transition, as was described previously in Malta(Reference Tessier and Gerber11).
Thus the aim of the present work was to assess the current MDP of the inhabitants of the Greek islands (in the eastern Mediterranean) and the Balearic Islands (in the western Mediterranean).
Subjects and methods
Balearic Islands sample
The sample of Balearic islanders (BI) was derived from a population-based, cross-sectional nutritional survey carried out in the Balearic Islands (Mallorca, Menorca, Ibiza and Formentera) between 1999 and 2000 (Nutritional Study of the Balearic Islands; ENIB). The target population consisted of all inhabitants living in the Balearic Islands aged 16–65 years, and the sample population was derived from residents registered in the official population census of the Balearic Islands. The sampling technique included stratification according to geographical area and municipality size (six strata), age (three strata) and sex of inhabitants, and randomization into subgroups, with Balearic Islands municipalities being the primary sampling units and individuals within these municipalities comprising the final sample units. Target eligibility criteria were being an apparently healthy man or woman aged 16–65 years. Pregnant women were not considered in the study. The theoretical sample size was set at 1554 individuals, who were contacted by telephone, informed about the objective of the study and sited in their house for the interview. One thousand two hundred individuals (77 % participation) agreed to participate. Non-participants were those potential subjects declining to be interviewed as well as involuntary non-participation due to census error caused by address changes, missing persons or unavoidable impediments to survey collaboration.
The ENIB study consisted of a dietary interview (semi-quantitative FFQ) and a questionnaire incorporating questions about age group and educational level (grouped according years and type of education: low, <6 years at school; medium, 6–12 years of education; high, >12 years of education). More details about the sampling procedure and study details have been published elsewhere(Reference Tur, Romaguera and Pons28, Reference Tur, Serra-Majem, Romaguera and Pons34–Reference Tur, Serra-Majem, Romaguera and Pons36). The study was approved by the Ethics Committee of Clinical Investigation of the Balearic Islands and the University of the Balearic Islands.
Greek islands sample
The sample of Greek islanders (GI) consisted of a sub-sample of the Greek component of the European Prospective Investigation into Cancer and Nutrition (EPIC–Greece). Greek EPIC participants were recruited from the general population during 1994–1999. Four Greek islands – three Aegean islands (Kastelórizo, Symi, Metilina) and one Ionic island (Medanisi) – were randomly selected to form part of the present study. The study populations were volunteers agreeing to participate; subjects were invited from the general adult population residing in a given town or geographical area. Participants were actively recruited, they had their EPIC study centre examination at enrolment and all completed an interviewer-administered questionnaire on diet and a questionnaire on lifestyle(Reference Riboli, Hunt and Slimani37). Individuals who agreed to participate signed an informed consent agreement. Target eligibility criteria were being an apparently healthy man or woman aged 16–65 years. The initial simple size consisted of 1408 individuals, but 1324 individuals completed the survey (94 % participation).
Each EPIC participant completed an extensive interviewer-administered questionnaire similar to that described above. More information about the study details can be found elsewhere(Reference Trichopoulou, Costacou, Bamia and Trichopoulos16, Reference Riboli, Hunt and Slimani37, Reference Costacou, Bamia, Ferrari, Riboli, Trichopoulos and Trichopoulou38). The study protocol was approved by the Ethics Committee of the International Agency for Research on Cancer and the Athens University Medical School.
Dietary intakes
Validated semi-quantitative FFQ that included 145 foods and beverages, as well as questions on usual cooking methods, fats used for frying, cooking and dressing, were used to assess usual food and beverage consumption during the previous year. The ENIB FFQ was designed on the basis of a validated FFQ(Reference Serra-Majem and Ribas39, Reference Serra-Majem40) used in other Spanish studies, modified by entering just regional Balearic recipes, and was validated in the pilot phase of the study(Reference Tur41). The Greek-EPIC questionnaire was validated in the pilot phase of the study(Reference Gnardellis, Trichopoulou, Katsouyianni, Polychronopoulos, Rimm and Trichopoulos42–Reference Slimani, Fahey and Welch44). The questionnaires were administered in the subject’s home by well-trained dietitians. In order to estimate volumes and portion sizes, the subjects were asked for the household measures, and standard portion sizes were used as references(Reference Tur41–Reference Slimani, Fahey and Welch44). Food items included in both FFQ were carefully grouped into nineteen food groups according to a common classification used in EPIC study(Reference Slimani, Fahey and Welch44): cereals (g/d), vegetables (g/d), fruits (g/d), potatoes and tubers (g/d), legumes (g/d), nuts (g/d), dairy products (g/d), meat and meat products (g/d), fish and shellfish (g/d), eggs (g/d), olive oil (g/d), seed oils (g/d), butter (g/d), margarine (g/d), sugar and confectionery (g/d), non-alcoholic beverages (ml/d), spirits (ml/d), beer (ml/d) and wine (ml/d). These food groups were ordered according to their plant or animal origin and their degree of food processing to facilitate the comparison of dietary patterns across islands. Data presented here were based on the data from the FFQ that overlapped both instruments (Greek-EPIC FFQ and ENIB FFQ).
Nutrient intakes were estimated using high-quality reference food composition tables specific to the country: Greece(Reference Trichopoulou and Critselis18, Reference Trichopoulou45) and Spain(Reference Ripoll46–Reference Mataix, Mañas, Llopis, Martínez de Victoria, Juan and Borregón49). Total energy intake was derived from the FFQ. Food and beverage consumption (g/d or ml/d) was adjusted to daily intakes of 4·2 MJ (1000 kcal) to make easy the comparison between GI and BI samples. In order to avoid respondent bias and increase the validity of the dietary measurements, individuals who showed an energy intake <3·25 MJ or >20·75 MJ were excluded from the analysis. After the exclusion, the final sample comprised 1315 individuals from the Greek islands and 1160 from the Balearic Islands.
Methods applied in the present work differed on the use of food composition tables specific to the country (Greece and Spain), the design of questionnaires specific to the country, and the final number of interviewees.
Mediterranean Diet Score
Adherence the traditional Mediterranean diet was assessed by a 10-point Mediterranean Diet Score (MDS) that included nine nutritional components characteristic of the Mediterranean diet: vegetables, fruit and nuts, cereals, legumes, fish and shellfish, moderate alcohol consumption, ratio of monounsaturated to saturated lipids, meat and meat products, and milk and dairy products(Reference Trichopoulou, Costacou, Bamia and Trichopoulos16, Reference Trichopoulou, Kouris-Blazos, Wahlqvist, Gnardellis, Lagiou, Polychronopoulos, Vassilakou, Lipworth and Trichopoulos26). This scoring method (MDS) was used to contrast the Mediterranean diet adherence between GI and BI populations.
According to previous data(Reference Panagiotakos, Milias, Pitsavos and Stefanadis29–Reference Rimm, Giovannucci, Willett, Colditz, Ascherio, Rosner and Stampfer32), a presumably beneficial effect on overall morbidity and mortality was attributed to vegetables, fruit and nuts, cereals, legumes, fish and shellfish, moderate alcohol consumption, and ratio of monounsaturated to saturated lipids, whereas a presumably detrimental effect on overall morbidity and mortality was attributed to meat and meat products, and milk and dairy products.
Values of 0 or 1 were assigned to each MDP component (except for ethanol intake) using as cut-off point for all characteristics the corresponding median values specific to each sex of both populations (GI and BI), as described elsewhere(Reference Trichopoulou, Costacou, Bamia and Trichopoulos16, Reference Trichopoulou, Kouris-Blazos, Wahlqvist, Gnardellis, Lagiou, Polychronopoulos, Vassilakou, Lipworth and Trichopoulos26). Persons with a below-median consumption of components with a presumably beneficial effect on overall morbidity and mortality were assigned a value of 0, whereas persons with consumption above the median were given a value of 1. In contrast, persons with a below-median consumption of components with a presumably detrimental effect on overall morbidity and mortality were assigned a value of 1, whereas persons whose consumption of these components was above the corresponding median were given a value of 0. For ethanol, a value of 1 was given to men whose consumption of ethanol was from 10 to <50 g/d, whereas for women the corresponding cut-offs were 5 and 25 g/d. For lipid intake, the ratio MUFA:SFA was used because monounsaturated lipids are consumed in much higher quantities in Greece and Spain than other types of unsaturated fat. The range of the MDS was 0 to 9, with higher scores indicating greater adherence to the Mediterranean diet. A value of 9 would be the optimal Mediterranean diet.
Sociodemographic variables
Sociodemographic variables considered in the present study were gender, age group (<35 years old, 35–50 years old, >50 years old) and educational level based on the highest school level achieved (none or primary education was codified as low, secondary education as medium, university studies as high educational level). These variables were the confounders in common to both studies (ENIB–Balearic Islands and EPIC–Greek islands).
Statistical analyses
Analyses were carried out with STATA version 8·0 (STATA Corp LP, College Station, TX, USA) and SPSS version 15·0 (SPSS Inc., Chicago, IL, USA) statistical software packages. Descriptive analysis relied on cross-tabulations, showing percentages within groups as well as group means and standard deviations. Differences among percentages were assessed using the χ 2 test; differences between means were analysed by ANOVA. To study the determinants of MDP adherence and the level of significance of differences in food patterns, multiple linear regression analyses (considering the simultaneous effect of age, sex, educational level and Mediterranean region) were performed.
Results
Table 1 shows mean values of the MDS stratified by sociodemographic characteristics. Both samples differed substantially in their sociodemographic traits. The mean age of the BI sample was 37·1 (sd 14·5) years, whereas that of the GI sample was 52·1 (sd 12·7) years (data not shown). Differences were also observed in educational level: 55·7 % of GI belonged to the lowest educational level but only 11·0 % of the BI sample was included in this educational group. Most of the BI sample (68·3 %) had a medium educational level. Mean MDS was 5·1 (sd 1·4) in the GI group and 3·3 (sd 1·2) in the BI group (P < 0·0001). Since MDS of 9 represents 100 % adherence to the MDP, these results translate into 57 % adherence to the MDP in the GI sample and 37 % adherence in the BI sample (data not shown). Therefore, the GI sample ate a more Mediterranean-like diet (+20 %) than the BI sample.
Table 1 Mediterranean Diet Score (MDS) stratified by sociodemographic characteristics: data from a sub-sample of the Greek component of the European Prospective Investigation into Cancer and Nutrition (1994–1999) and the Nutritional Study of the Balearic Islands (1999–2000)

†All differences between percentages of Greek and Balearic individuals in each sociodemographic group were statistically significant (P < 0·0001).
‡P values show the level of statistical significance of the observed differences in mean MDS among sociodemographic groups within each Mediterranean region.
§P value shows the level of statistical significance of the observed difference between mean MDS values of Greek islanders and Balearic islanders.
Age was an important determinant of adherence to the MDP in both samples. The older the population, the higher was the MDS. This association remained significant after adjusting for sex, educational level and Mediterranean region (Table 2). Females showed a higher adherence to the MDP in BI but not in GI. In the unadjusted analysis, individuals belonging to the lowest educational level showed a greater adherence to the MDP in both BI and GI samples (Table 1). However this association was not longer significant in the adjusted analysis, since the relationship between MDS and educational level had been confounded by differences in age among educational levels (Table 2).
Table 2 Multiple regression-derived coefficients (β) and standard errors of sociodemographic predictors of Mediterranean Diet Score in each Mediterranean region: data from a sub-sample of the Greek component of the European Prospective Investigation into Cancer and Nutrition (1994–1999) and the Nutritional Study of the Balearic Islands (1999–2000)

Figure 1 shows BI and GI sample distribution in each MDS category adjusted by age. Both samples showed a fairly normal distribution along the 10-point MDS. However, the BI distribution was shifted to the left (lower scores) whereas the GI distribution was centred on the right (higher scores).
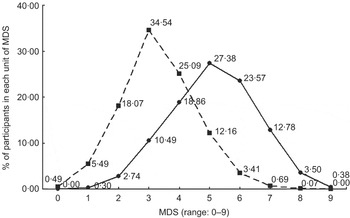
Fig. 1 Distribution of 2475 participants by Mediterranean region (![]() , Balearic Islands;
, Balearic Islands; ![]() , Greek islands) and single units of the Mediterranean Diet Score (MDS) adjusted by age: data from a sub-sample of the Greek component of the European Prospective Investigation into Cancer and Nutrition (1994–1999) and the Nutritional Study of the Balearic Islands (1999–2000)
, Greek islands) and single units of the Mediterranean Diet Score (MDS) adjusted by age: data from a sub-sample of the Greek component of the European Prospective Investigation into Cancer and Nutrition (1994–1999) and the Nutritional Study of the Balearic Islands (1999–2000)
Table 3 shows the comparison of food patterns (g/d or ml/d calculated for an energy intake of 4·2 MJ or 1000 kcal) in the GI and BI samples by sex. The consumption of most food groups differed greatly between GI and BI samples (P < 0·0001, analysis adjusted for age and educational level) with the exception of dairy products (P = 0·619 for males and 0·505 for females), butter (P = 0·408 for males and 0·840 for females), margarine (only males, P = 0·256), cereals (only females, P = 0·107) and spirits (only females, P = 0·736). Within the vegetal food groups, the GI sample showed greater intakes of vegetables, fruits, and potatoes and tubers than the BI sample, whereas BI individuals had a higher consumption of legumes, nuts and cereals (the latter only males) than GI individuals. GI consumption of animal products (fish, meat) was greater than that of BI. The intake of sugar and confectionery, and non-alcoholic beverages was higher in BI than in GI. The GI sample showed a higher intake of olive oil than the BI sample, but the latter’s consumption of seed oils and margarine (only females) was greater than that of GI. Males’ intake of spirits, wine and beer was greater in GI than in BI.
Table 3 Comparison of food patterns between Balearic and Greek islanders: data from a sub-sample of the Greek component of the European Prospective Investigation into Cancer and Nutrition (1994–1999) and the Nutritional Study of the Balearic Islands (1999–2000)

*P < 0·05 (all P values were corrected by sequential Bonferroni test to control type I error).
†Daily consumption was adjusted for an energy intake of 4·2 MJ (1000 kcal).
‡Cereal group includes flour, flakes, starches, pasta, rice, other grain, bread, crispbread, rusks, breakfast cereals, biscuits, dough, pastry, etc.
Discussion
In the Mediterranean countries at the beginning of the 1960s, plant foods especially vegetables, cereals and pulses were traditionally highly consumed, whereas animal products were consumed in moderate amounts at each meal(Reference Trichopoulou4). From 1961 to 2001, the availability of fruits was high in Greece and Spain, the availability of vegetables and olive oil was high in Greece and intermediate in Spain, whereas the availability of cereals and fish was high in Spain; lately, the availability of meat and derivates has increased dramatically both in Greece and Spain. Although these figures show a trend towards a Western diet, Spain and particularly Greece still show a Mediterranean pattern of lipid intake that can be clearly differentiated from dietary patterns found worldwide(Reference Garcia-Closas, Berenguer and González50, Reference Leonhäuser, Dorandt, Willmund and Honsel51).
In comparison to the dietary patterns observed in Greece and Spain, several differences in the Greek islands and the Balearics have been observed. Greek islanders consumed more alcoholic beverages and less cereals, potatoes and tubers, legumes, dairy products, meat and meat products, fish and seafood, and non-alcoholic beverages than the overall Greek population(Reference Elmadfa and Weichselbaum12). Balearic islanders consumed more vegetables, nuts, sugar and confectionery, and non-alcoholic beverages, but less cereals, fruits, potatoes and tubers, legumes, dairy products, meat and meat products, fish and seafood, eggs, and alcoholic beverages than the overall Spanish population(Reference Aranceta, Serra-Majem, Perez-Rodrigo, Llopis, Mataix, Ribas, Tojo and Tur52). Differences in food patterns were also observed between the GI and BI samples in the present study. BI consumption of legumes, nuts, seed oils, sugar and confectionery, and non-alcoholic beverages was higher than GI, whereas the GI diet was richer in fruit, vegetables, potatoes, olive oil, animal products and alcoholic beverages.
Since Key’s first observations(Reference Keys and Grande1), the Mediterranean diet has been under scrutiny by researchers and public health specialists worldwide for its health-promoting qualities(Reference Ferro-Luzzi and Branca20). Recent studies, capturing the evidence accumulated over the past four decades, have documented that the traditional MDP meets several important criteria for a healthy diet(Reference Trichopoulou and Vasilopoulou2–Reference Trichopoulou4, Reference Moreno, Sarria and Popkin5, Reference Corpet and Gerber14–Reference Martinez-Gonzalez, Fernandez-Jarne, Serrano-Martinez, Marti, Martinez and Martín-Moreno23). There is sufficient evidence that the Mediterranean diet positively influences longevity, but also that an optimal diet for the prevention of both CHD and cancer is likely to overlap extensively with the traditional Mediterranean diet(Reference Trichopoulou4, Reference Trichopoulou and Critselis18). Accordingly, several attempts to conceptualize the Mediterranean diet have been reported and several Mediterranean dietary scores have been developed and evaluated(Reference Trichopoulou, Kouris-Blazos, Wahlqvist, Gnardellis, Lagiou, Polychronopoulos, Vassilakou, Lipworth and Trichopoulos26–Reference Tur, Romaguera and Pons28).
Our results on adherence to the MDP showed that neither Greek islanders nor Balearic islanders follow the optimal Mediterranean diet, but the mean dietary pattern of three-fifths of Greek islanders (57 % adherence to MDP) and two-fifths of Balearic islanders (37 % adherence to MDP) is Mediterranean. These results agree with previous works(Reference Scali, Richard and Gerber8–Reference Tessier and Gerber11) pointing out the trend for MDP disappearance in several Mediterranean regions.
Because of isolation due to naturally defined borders, the Mediterranean islands would seem appropriate locations for retaining healthy food habits. Thus it is surprising that the MDP was not as prevalent as one might expect. It is quite difficult to know the reason for the different degrees of MDP adherence among Greek and Balearic islanders, since it could result from variations of dietary patterns across cultures but also external influences on dietary patterns.
One external influence might be the influx of tourism on the islands, since this represents the arrival of foreigners, the establishment of non-native individuals and the subsequent introduction of new foods, new ways to cook and new food habits. The percentage of non-native individuals in the Greek and Balearic samples seems to be not important, since it was low (4 %) when the surveys were done, but the intensity of tourism industry establishment may represent an important factor of transformation of traditional habits of islanders. In 2007, 10.5 million tourists visited the Balearic Islands and 8 million visited all Greek islands, whereas the number of inhabitants was 955 000 in the Balearics and 1 190 000 in the Greek islands (including Crete)(33). This means that tourism is the main (or the sole) industry in the islands, which could affect island life to different degrees. However, it is likely that tourism has had a tremendous impact on many aspects of society, including food habits, as observed previously in other Mediterranean islands, i.e. Sardinia and Malta(Reference Tessier and Gerber11). In Sardinia, food changes have occurred within the frame of the Mediterranean food culture, whereas in Malta the Anglo-Saxon cultural context due to past colonial presence, migration and tourism has had a deep impact on food habit changes, by promoting excessive consumption of meat and foods rich in fats and sugar(Reference Tessier and Gerber11). All these results show that a nutrition transition is being progressively implanted on the Mediterranean islands, but at different speeds.
Our study found that age and educational level were important determinants of the adherence to the MDP in the whole pooled sample and in western and eastern Mediterranean samples separately. These results agree with previous studies conducted in Spain and Greece(Reference Sanchez-Villegas, Martínez, De Irala and Martínez-González27, Reference Tur, Romaguera and Pons28, Reference Serra-Majem and Ribas39, Reference Trichopoulou, Orfanos and Norat53, Reference González, Argilaga and Agudo54) which revealed the loss of the MDP in young generations and the greatest adherence to the MDP in people older than 50 years.
In light of these findings, even in areas where one might expect to see traditional Mediterranean eating patterns, there appears to be considerable variability in actual practices. This variability will be important to understand, particularly if such findings are to be used to inform public health policy and clinical practice.
However, several questions still remain unsolved. Is the MDP an integral entity, or the sum of identifiable components that can and should be separately considered in the development of guidelines? Is the MDP or its major components transferable to populations living far from the Mediterranean area? Answering these questions would be important for scientific and public health policy reasons. Our study may contribute useful information to enable these questions to be answered appropriately and completely at some future date.
Limitations of the current approach
Several limitations of the study must be considered. First, the sociodemographic characteristics of the BI and GI samples were quite different, GI individuals were older and less educated than BI individuals; however, all statistical analyses carried out to assess the level of significance of the observed differences in MDS and food patterns between regions were adjusted for age, sex and educational level. Second, participants in the Greek study were volunteers whereas participants in the Balearic study were selected randomly. Third, the time frames of both studies were also slightly different (the GI sample was recruited during 1994–1999 while the BI nutritional study was conducted between 1999 and 2000). Fourth, over the years, researchers have come to recognize that the dietary assessment method used (FFQ) usually tends to overestimate food and nutrient intake, and the reported values from FFQ are subject to substantial error, both systematic and random. Nevertheless, taking into account the well-known limitations of the use of FFQ, we absolutely agree with the opinion of previous authors(Reference Willett and Hu55, Reference Willett and Hu56) who defend the use of FFQ with firm and clear statements. Finally, the absence of a broader array of covariates prevents more formal modelling of the determinants of MDP adherence.
Conclusions
The diet of Spanish (Balearic) islanders seems to differ more markedly from the traditional MDP than that of Greek islanders, despite the fact that Spanish islanders’ diet still preserves some Mediterranean characteristics. Given the growing available evidence on the beneficial effects of the traditional Mediterranean diet on health(Reference Trichopoulou4, Reference Trichopoulou, Costacou, Bamia and Trichopoulos16, Reference Gnardellis, Trichopoulou, Katsouyianni, Polychronopoulos, Rimm and Trichopoulos42), the loss of the MDP in Greek and Spanish Mediterranean islanders should be seriously considered by public health authorities. To avoid and stop the progression of the nutrition transition’s consequences on health, it seems sensible to concentrate efforts on the promotion and recuperation of traditional dietary patterns across the Mediterranean area.
Acknowledgements
Source of funding: The ENIB study was granted by the Spanish Ministry of Health (Projects 97/0007-00, 97/0007-01, 02-1593 and 05-1276). EPIC–Greece was coordinated by the International Agency for Research on Cancer and supported by the Europe against Cancer Programme of the European Commission, the Greek Ministry of Health and the Greek Ministry of Education. The Balearic Islands’ Ministry of Economy, Finance and Innovation supported a PhD fellowship to D.R.
Conflicts of interest: None of the authors had any conflicts of interest.
Authors’ contributions: D.R. performed the data analyses. C.B. evaluated the data analyses and the interpretation of the results. A.P., J.A.T. and A.T. conceived and designed the study, and reviewed the manuscript, the data analyses and the interpretation of the results. A.P., D.R., A.T. and J.A.T. wrote the manuscript.




