



The COVID-19 pandemic has changed the way humans inhabit physical spaces since early March 2020. Practices such as social distancing, wearing masks in congested public spaces, restricted entry to indoor venues, and a reduced occupancy in all public transport including air travel have become the new normal. Shifting contours of the urban space are making it imperative for us to reimagine cities and reprioritize our urban planning goals.
Urban centers have borne the brunt of casualties in the current pandemic. This has raised long-term fears about the viability of high-density habitation and public transport usage as they may lead to the spread of contagions. However, nuanced evaluations have shown that the experience of urban centers with the pandemic is highly varied and there are ways to build urban resilience through effective urban management.
This intelligence briefing paper argues that there is little evidence that urban density alone is the culprit in the spread of COVID-19. Our analysis of extant literature reveals a multitude of other factors such as urban inequality especially along racial lines, income, and living conditions that have a high correlation with the spread of disease. We present the case study of Karachi, Pakistan, one of the largest mega-cities in the developing world with around 20 million inhabitants, to further solidify our argument. We also consider some of the key debates around density, mobility and environment, and decentralization as city governments confront this public health crisis. Finally, we offer ways in which inclusivity in the urban planning process could be a sterling feature of the post-COVID urban recovery efforts and a way to combat inequality in cities.
1. Reconfiguring urban life: the density debate
Population density has been a key topic in urban studies since the time of the industrial revolution. The simplest way to calculate urban density is to measure the number of people per unit area. However, this definition of density is often confused with ‘crowding’. Crowding occurs when people live together in a space that is designed for a smaller number of occupants and is different from urban density which assumes people living close but in uncrowded conditions (Wiener & Iton, Reference Wiener and Iton2020).
In the realm of public health, density has always been a cause of concern as ‘negative effects of proximity if not properly managed can destroy the quality of life in any urban area’ with contagious diseases as an ‘urban externality’ (Glaeser, Reference Glaeser2011, p. 112). A preliminary study on the relationship between density and COVID-19 by Hamidi et al. (Reference Hamidi, Sabouri and Ewing2020) shows that density is not linked to the rates of COVID-19 among US counties. Their findings suggest that connectivity matters more than density, and larger metropolitan areas with counties connected to one another are at a higher risk (Hamidi et al., Reference Hamidi, Sabouri and Ewing2020). Additionally, Bozikovic (Reference Bozikovic2020) in his article cites a World Bank study of 248 cities which illustrates that the densest of the country's cities had some of the lowest per-capita rates of transmission.
So, if urban density is not the cause of concern, what are some other factors that can result in the spread of COVID-19? Literature suggests that household composition, income inequalities, and inadequate infrastructure for lower income neighborhoods, social class, race, and the intersection of all the aforementioned factors have helped increase the transmission of the virus. Both infections and death are disproportionately related to class and race. For instance, early data indicated that in the UK, 35% of the first 2,249 patients with confirmed COVID-19 were non-white (Ro, Reference Ro2020). Further, minority racial populations who are already economically vulnerable have a higher incidence of COVID-19 and their economic consequences are more severe too. McKinsey and Company reports that ‘39% of jobs held by black workers, 7 million jobs in all, are vulnerable as a result of the COVID-19 crisis, compared with 34% for white workers’. Additionally, ‘40% of the revenues of black-owned businesses are in the 5 most vulnerable sectors – including leisure, hospitality and retail – compared with 25% of the revenues of all US businesses’ (Blow, Reference Blow2020). Low-income populations are also more likely to live in crowded households with inadequate infrastructure, which makes them more susceptible to the contagion. Thus, inadequate socioeconomic policies have a bigger role to play in exacerbating the pandemic than urban density alone.
Government responsiveness to the pandemic is another factor that determined the variations in the spread of COVID-19. For instance, Hanoi city in Vietnam was able to contain the spread of COVID-19 by taking policy actions to restrict travel and launch rapid testing, contact tracing, and quarantining measures. Conversely, cities such as New York in the USA were slow to react which led to overutilization of health services and a much higher death toll. Also, governments in Asian cities such as Hong Kong that had previously been exposed to SARS in 2003 were better prepared to mandate masks. This is in contrast to New York, where delayed implementation of a mask policy was in part a result of having no recent experience with such a contagious airborne disease (Bai et al., Reference Bai, Nagendra, Shi and Liu2020). These examples show that the effects of density do not follow the trend that the proponents of de-densification predict. Areas and localities with systems that could mobilize quicker did better in terms of controlling transmission, as compared to equally dense or more dense areas. Robert Steuteville, editor of the journal Public Square, comments that these arguments backed by data obfuscate the idea that there is an obvious relationship between density rates and transmission rates and disproves the dominant ‘density is dangerous narrative’ (Holland, Reference Holland2020).
In fact, advocates of urban density contend that density is good for public health due to the concentration of health care resources, and efficient emergency services (Wiener & Iton, Reference Wiener and Iton2020). Density creates socially sustainable neighborhoods, inclusive communities, more vibrant economies, and lowers costs of living for residents (Newman & Hogan, Reference Newman and Hogan1981; Raman, Reference Raman2010; Shaw, Reference Shaw1989; Waters, Reference Waters and Simon2016, p. 19). Moreover, those who are cautious in placing all the responsibility on density point toward entrenched inequalities as a huge determinant of public health concerns. Indorewala and Wagh (Reference Indorewala and Wagh2020) argue that ‘our cities are vulnerable, not because they have high aggregate densities, but because they are highly unequal in terms of living conditions, services, incomes and access’. High-risk populations in India are victims of structural inequality that results in unequal neighborhoods and crowded homes that lack basic infrastructure and provision of essential services. These issues need to be recognized by policy makers so that social inequalities are not aggravated by the pandemic and there is no acceleration of existing negative trends that segregate urban spaces based on class. There is a need for urban planning to be inclusive so that public health and economic crises can be managed effectively in the future.
Indorewala and Wagh (Reference Indorewala and Wagh2020) also suggest that the COVID-19 crisis is not a crisis of the city but a crisis for a certain kind of city. This kind of city is steeped in inequality and has weak public sector institutions that have failed to account for citizen's problems and anticipate their needs. Harvey (Reference Harvey2008) posits that urbanization has always been a class phenomenon and such an analysis shows merit at a time when the effects of a public health emergency are being felt across areas with different income levels in very different ways. So, instead of only focusing on negative externalities of density, there is a need for initiating a dialogue on vulnerabilities in cities that can worsen a public health crisis.
2. The case of Karachi
We obtained Union CouncilFootnote i level dataFootnote ii from the administrative districts in Karachi city, Pakistan to gain insight into the correlation between density and the spread of COVID-19. Karachi is the largest metropolitan city of Pakistan with around 20 million people and the city which witnessed the highest number of COVID-19 infections. Figure 1 indicates while the highest positive cases are largely concentrated in Karachi South, they are not found in the densest areas. Of the 5 hotspots, in terms of number of cases that are signified by black dots, none are in the maximum density zone. The concentration of COVID-19 in Karachi South may be attributed to various factors. For instance, one badly hit neighborhood is the Saddar area which has a high concentration of commercial activity and human interaction. Also, some of the neighborhoods with a higher prevalence of COVID-19 infections are relatively more well-off economically and people of these areas may be opting more for voluntary testing (Twohey et al., Reference Twohey, Eder and Stein2020). Conversely, there has been a tendency in many parts of the country, especially in marginalized segments, to avoid undergoing COVID-19 tests due to fear of being sent to isolation facilities by the government (Fear of testing, 2020). Therefore, inequality in terms of access to healthcare as well as financial means to avail testing shapes the data we have. Third, there was a higher presence of COVID-19 in some areas where the concentration of healthcare facilities is high. So, the reporting of location of patients may not have been recorded accurately in other zones, leading to present findings. However, there has not been any noticeable change in hospitalization from the areas with lower prevalence; the testing–density relationship is still plausible. Although no conclusive findings can be made regarding the reasons for the presence of higher COVID-19 infections in a few neighborhoods, the data help us understand and supplement the idea that density is not the only factor for the spread of the pandemic. So, it helps dispel the notion that we must advocate for anti-density policy. Figure 2 shows the number of COVID-19 cases plotted against population density, corroborating the earlier evidence that high population density does not necessarily result in higher transmission of the virus.
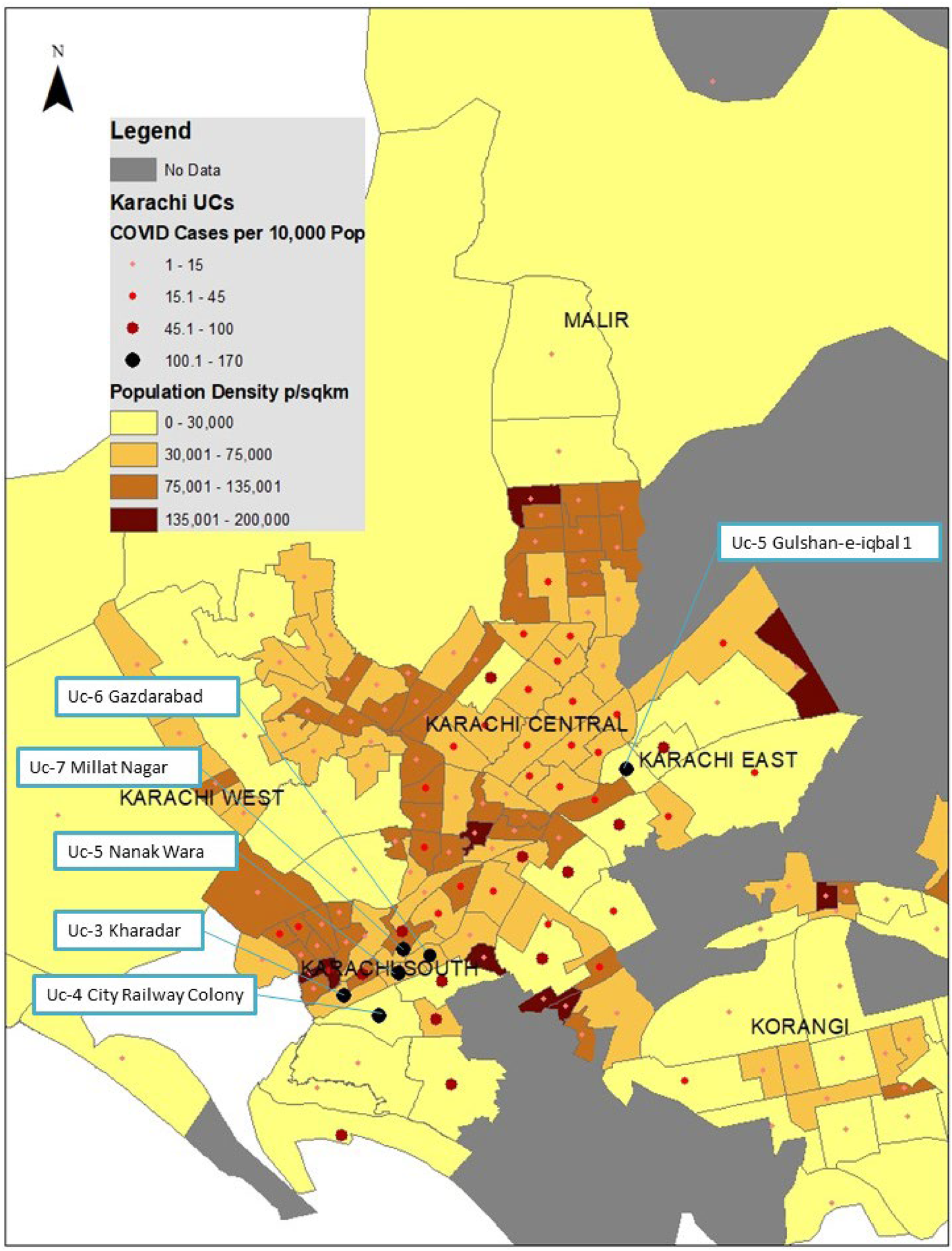
Fig. 1. Heat map of density and COVID-19 infections at Union Council level in Karachi, Pakistan.
Source: Developed by authors based on data of COVID-19 infections obtained from administrative districts of Karachi city.
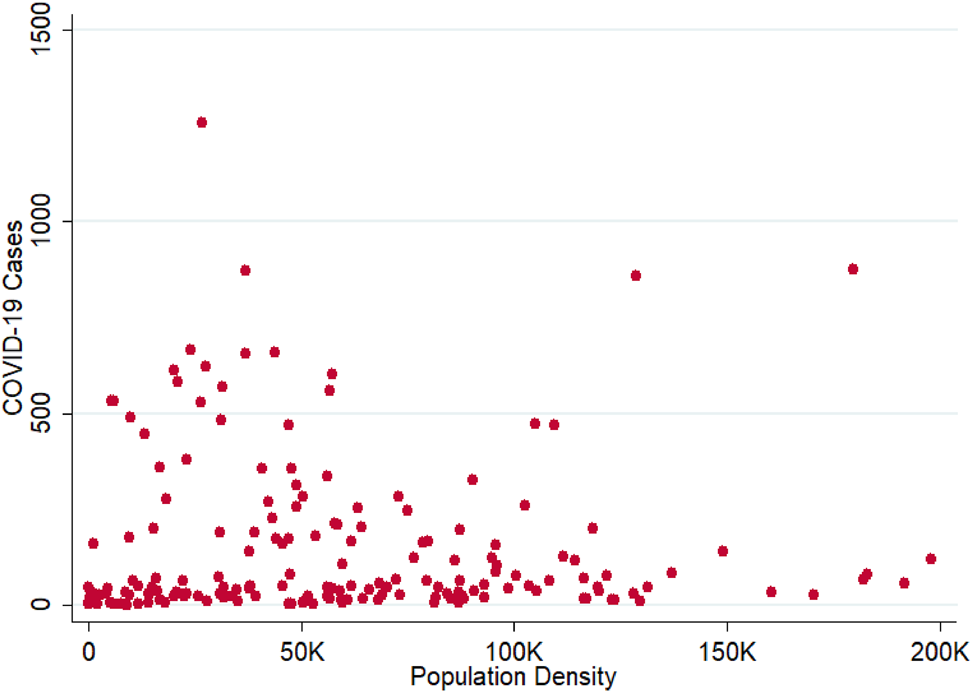
Fig. 2. Number of COVID-19 cases vs. population density at Union Council level in Karachi, Pakistan.
Source: Developed by authors based on data of COVID-19 infections obtained from Administrative districts of Karachi city.
To further contextualize the case of Karachi, reference can be made to the work carried out by the Karachi Urban Lab. This field-oriented research organization has noted that households in Karachi cohabit 8–9 people on average, living in areas as small as 20 yards (Karachi Urban Lab, 2020). Thus, household members cannot practice social distancing when forced indoors during lockdown. Crowded households along with other living conditions and lack of basic amenities severely impact the ability to implement preventative measures. Figure 3 shows a plot of COVID-19 cases against population density categorized by socioeconomic status. The graphs demonstrate that people belonging to low, low to middle, and middle socioeconomic classes have (1) a higher number of COVID-19 cases in general and (2) relatively higher COVID-19 cases at low population densities. This again confounds the assumption that high population density leads to higher transmission, and implies that other factors such as inequality, income, and living conditions may be more pressing issues in this pandemic. Therefore, King et al. (Reference King, Orloff, Virsilas and Pande2017) advocate ‘comprehensive approaches’, which include social programs in addition to infrastructure upgrading for such housing settlements.
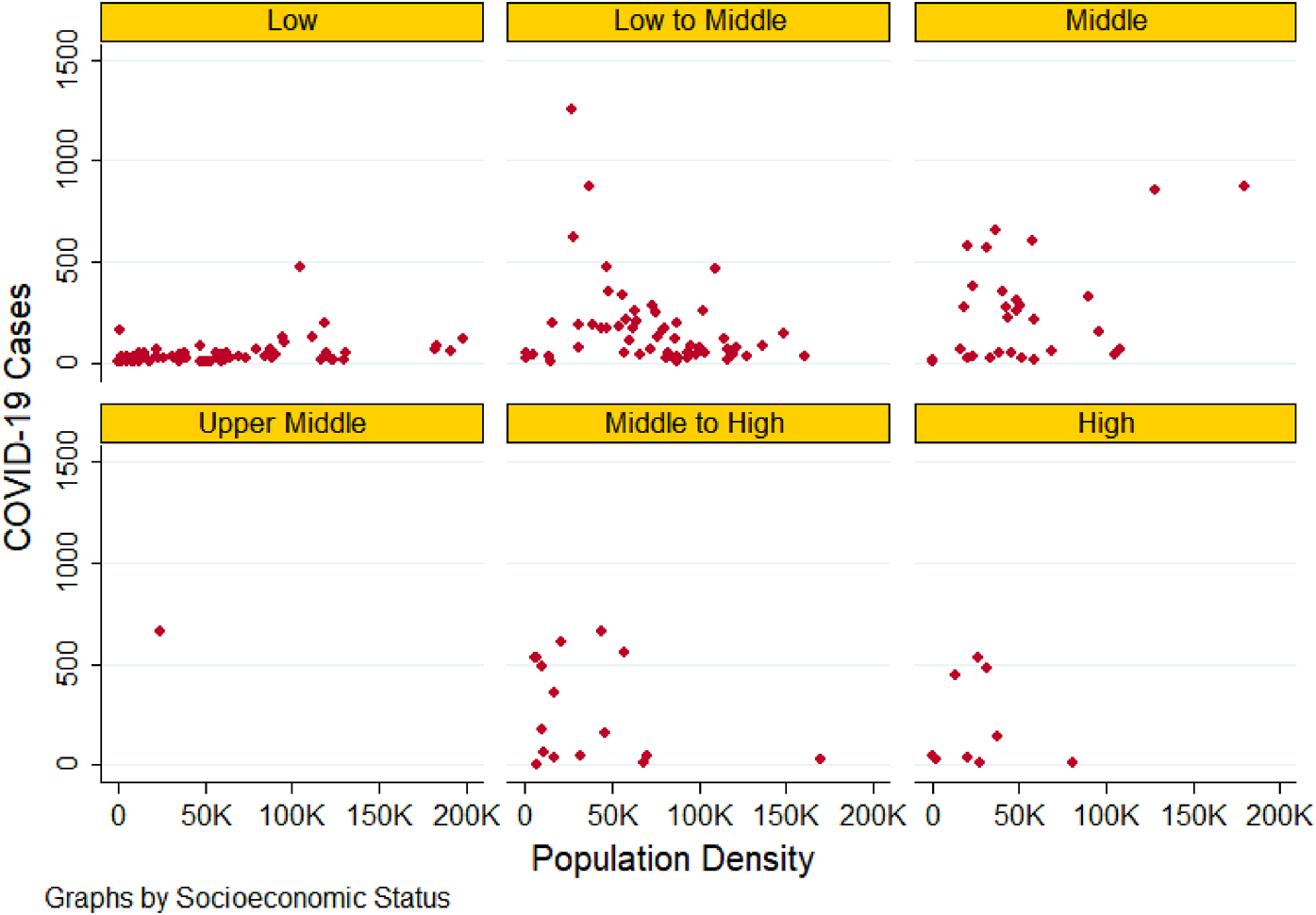
Fig. 3. Number of COVID-19 cases vs. population density segregated by socioeconomic class at Union Council level in Karachi, Pakistan.
Source: Developed by authors based on data of COVID-19 infections obtained from administrative districts of Karachi city.
3. Public spaces and mobility
There is a psychological toll and aversion to crowds that is deeply impacting the use of public spaces and modes of transport. Historically, pandemics have played a role in shaping cities by bringing major transformations in areas such as water and sanitation, industry pollution, and other policy changes. For instance, the bubonic plagues in medieval Europe led to measures that restructured the economy, and the Cholera outbreak led to global conversations on sanitation and public health (Florida, Reference Florida2020). Similarly, during this crisis, some authors such as Honey-Roses et al. (Reference Honey-Roses, Anguelovski, Bohigas, Chireh, Daher, Konijnendijk and Nieuwenhuijsen2020) are suggesting we may see the growth of ‘micro mobility’ with vehicles such as scooters and bicycles replacing other close contact modes such as cars and public transport. Pedestrians and cyclists are replacing cars and crowded public transport in many parts of the world. Bogota, Colombia has opened temporary bike lanes while New York has begun trials to set up miles of ‘open streets’ to ease crowding in parks. Cities such as Auckland, Mexico City, and Quito are among the dozens of others in the world experimenting with similar measures. Other policies being implemented include changing traffic crossing buttons to ensure less contact with surfaces. France is going as far as to set up pop-up bike lanes to change car-dominated traffic flows and stress the merits of green spaces (Holland, Reference Holland2020). Citizens and governments alike are expressing their desire to rethink cities around people rather than cars to maintain the momentum of the significant drop in carbon emissions during the lockdown. For instance, Milan's Head of City Mobility, Marco Granelli, has expressed the desire to change car-oriented policies in the face of the crisis (Dans, Reference Dans2020).
Perhaps the pandemic can serve as the catalyst for a move toward greener, more eco-friendly cities, given the visible effects lockdown has had on air pollution and even animal life. All these changes will also be taking place in the context of greater comfort level among employers for working from home or hybrid office use patterns. In the tech industry particularly, large-scale surveys conducted across companies such as Amazon and Microsoft indicate many prefer work from home, which may prompt a long-term shift toward this work culture and reduce congestion on roads (Kolakowski, Reference Kolakowski2020b). Mark Zuckerberg from Facebook had announced as early as May 2020 that even after the pandemic the company would allow employees to work from home and embrace remote working as a new trend (Kolakowski, Reference Kolakowski2020a). Gallup studies that analyze policies of more than 650 Chief Human Resource Officers' responses to the pandemic found changes in management and communication, indicating a long-term change in the norms governing workers behaviors (Emond & Maese, Reference Emond and Maese2020). Some of these changes are thought to be permanent, for example, relaxed dress codes and business hours, and changes in ideas of what constitutes professional behavior, as shown by pets or children featuring in workplace videoconferences (Emond & Maese, Reference Emond and Maese2020). These also indicate the emergence of more personalized work relationships that are likely to change the social fabric of our society. Thus, urban policymakers must move at the same pace at which the world around us is changing and design cities that are embracing new modes of travel and social interaction.
4. Ideas for reimagining cities
COVID-19 has sensitized the world to a range of neglected issues in sustainable urban planning. Thus, salient parameters of the recovery of urban centers should consider the following factors:
4.1 Inclusivity in planning
Inclusivity in planning entails developing cities that can be more receptive to providing opportunities for all genders, lower-income populations, minorities, and people with disabilities. This can start with engaging vulnerable communities in urban planning and giving weight to their perspectives in policymaking (Coda, Reference Coda2020). For instance, we can learn a lot from disability and access literature since disability-friendly measures such as wider store aisles for wheelchairs, contact-less surfaces, and wider spaces in public transport allow for ease in implementing social distancing measures and can mitigate the risks of COVID-19 transmission (Keegan, Reference Keegan2020). The pandemic has highlighted that diversity in planning establishes legitimacy and contributes to the effectiveness of planning and planning thought (Sweet & Etienne, Reference Sweet and Etienne2011).
4.2 Neighborhood government empowerment
The importance of neighborhood-level governance has reemerged after COVID-19 as city administrations across the world had to make decisions about neighborhood-level lockdowns and contact tracing. Germany makes for an important case study to understand the merits of such governance since it has 400 different health offices at the municipality and rural district level who are spearheading efforts to make testing and other health services accessible (Oltermann, Reference Oltermann2020). Decentralization and transfer of powers and functions at neighborhood level can lead to faster responses by healthcare organizations and ensures local community participation. This is also crucial to improve accountability, strengthen health literacy, and formulate policies that are reflective of local needs (Kickbusch & Gleicher, Reference Kickbusch and Gleicher2012).
Another example is the formation of Neighborhood Health Action Centers by the New York City Department of Health and Mental Hygiene in 2016–17. This was a place-based model designed to cater to the historic inequities in the city. Such models, through information and resource sharing, are found to encourage continuous and organic collaboration within and beyond the councils and include external community organizations such as New York City agencies which aid in health services delivery (Dannefer et al., Reference Dannefer, Wong, John, Gutierrez, Brown-Dudley, Freeman, Roberts, Martins, Napier, Noyes, Seoh, Bedell, Toner, Easterling, Lopez, Manyindo and Maybank2019; Pierre et al., Reference Pierre, Letamendi, Sleiter, Bailey, Dannefer, Shiman and Sierra2020).
Similarly, Bai et al. (Reference Bai, Nagendra, Shi and Liu2020) discuss how local communities and other organizations fill in the gaps in leadership from the top. They point to Brazil's G10 Favela's community leaders' exemplary work as well as collaboration between the municipality and local low-cost private-health practitioners that capped the virus's spread in the Dharavi slum in Mumbai. We could speculate that if such neighborhood-level initiatives were prevalent in cities such as Karachi, where smart lockdowns were pioneered, the pandemic could have been significantly curtailed. Smart lockdowns targeted small localities rather than the city at large to minimize economic hardships on citizens keeping in mind economic inequalities and the daily wage economy. As these lockdowns relied heavily on community support, learning from examples of neighborhood government and local community cooperation during the pandemic is particularly useful.
4.3 Urban mobility and climate-friendly recovery
COVID-19 offers ‘a new baseline of what can be achieved digitally’ in various realms such as remote work, education, and even shopping (Jauregui, Reference Jauregui2020). This new baseline allows us to think of measures in urban mobility and climate-friendly recovery that we can implement even after the public health emergency subsides. For instance, making streetscapes more suitable for pedestrians, bicyles, and electric scooters can improve mobility and environment in cities. Vehicle to grid technology could also be upscaled in this context to ensure e-mobility is best optimized with renewable energy sources (Budd & Ison, Reference Budd and Ison2020; Khan et al., Reference Khan, Kadir, Mahmood, Ibne Alam, Kamal and Al Bashir2019). However, the need for people to feel safe in using public transport and living in high-density neighborhoods is paramount in assuring that the post-COVID era does not lead to individual vehicle usage increase or to less dense habitation. The ability of more individuals to work from home may also have important long-term climate change implications in terms of reducing transport emissions. The urban core of cities needs to remain attractive for human habitation if we are to prevent urban sprawl. It may also be possible that polycentric clusters of micro-cities develop where people do not need to commute due to a change in work culture. However, all telecommuting will be dependent on having excellent Internet and electricity infrastructure that will have its own initial carbon footprint.
5. Conclusion
Cities have endured pandemics in the past and been able to innovate and survive. The current test of urban resilience has come at a time of unprecedented technological advancement that has allowed for various adaptation mechanisms that can aid urban recovery. Density, mobility, and decentralization are three factors that must be managed carefully across urban cityscapes. Urban policies during these times must address social inequalities that determine access to healthcare during the pandemic. Although the data do not lead us to derive a causal relationship between any one factor as a mechanism in urban disease spread, it helps us thwart the idea of urban density as the only factor increasing the spread of COVID-19. Thus, cities in developing countries need to focus on developing resilience through adopting strategies that promote inclusion and equal resource distribution when building new infrastructure or developing urban spaces. This will help them face a similar public health crisis head on in the future.
Data
Datasets are available from the authors upon request.
Acknowledgements
We are grateful to administrative districts of Karachi city for providing us with Union Council Level data of COVID-19 infections. Sana Riaz provided research support to develop the heat map (Figure 1).
Author contributions
IK and MNI conceived the study and worked on the initial draft. SHA provided the review and structuring of the paper and guidance for collecting and analyzing new datasets. The collection and analysis of these datasets was done by IK and MNI. SK edited the paper, including new analysis and content, before submission to the journal.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflict of interest
None.




 Open access
Open access